Hip fractures represent a major healthcare concern, as over 300,000 adults are hospitalized for hip fractures every year. Additionally, hip fractures present a significant issue in terms of reduced functionality, morbidity, and mortality. It is estimated that the one-year mortality rate following a hip fracture may be as high as 58%. Pain control for hip fractures almost always begins in the emergency department (ED). Pain control has traditionally been accomplished by parental opioid medications, however with the recognition of many adverse effects and the heightened awareness of the opioid crisis, there has been a shift towards multimodal pain control for acute pain in the ED. Many clinicians have begun to utilize regional anesthesia in the ED for control of hip fracture pain. Despite this growing trend, there have been no large-scale randomized clinical trials to provide a universal policy or standard of care statement. This literature review was designed to provide an encompassing evaluation of the current literature comparing the potential use, efficacy, and safety of regional nerve blocks to traditional parenteral pain medications for hip fractures in the ED. Through this review, we have gained insight that regional anesthesia may offer a more rapid, efficacious, and safe alternative to pain control in patients with hip fractures, when compared to traditional modalities of pain control. This review has provided some support for the use of regional nerve blocks in the ED, as this practice may improve many clinically relevant and patient oriented aspects of ED hip fracture care.
INTRODUCTION
Hip fractures represent a major healthcare concern for adults, as every year it is estimated that over 300,000 people age 65 and older are hospitalized for hip fractures.4 As the baby boomer generation continues to age, this number is expected to grow substantially, with estimates of greater than 800,000 hip fractures per year by 2030 to 2040.10 It is well supported that hip fractures not only greatly reduce the functional status of patients, but also markedly increase the risk of mortality and significant morbidity. The one-year mortality rate following a hip fracture has been reported as high as 58%.10
Initial pain control for hip fractures almost always begins in the emergency department (ED). The inherent distractions and busy environment of the ED setting highlight the need for a modality that provides effective pain control with limited adverse effects. Reliability of the modality is also crucial, as patients with hip fractures require aggressive pain control. Traditionally, this has been accomplished by parental opioid medications; however, in terms of morbidity, it is well known that opioid medications place patients at a higher risk for delirium, respiratory depression, and addiction. Pain management research also suggests these medications may also indirectly lead to other adverse effects such as pressure ulcers, infections, and increased hospital length of stay.2
With the heightened attention to the opioid crisis, a push for multimodal pain control has been initiated. There has been an increasing amount of literature published on performing regional anesthesia for acute pain control in the ED. Additionally, the widespread use of ultrasound in the ED, has fostered an increase in the performance of regional nerve blocks for hip fractures. The ability to directly visualize anatomical landmarks and anesthetic deposition with ultrasound while performing regional nerve blocks has driven the thought of increased safety and speed. However, in some areas of medicine ultrasound may not be readily available, or the skillset required to use ultrasound is lacking. Regardless, many clinicians have begun to adopt the practice of using regional anesthesia in the ED for hip fractures. Despite this growing trend, there have been no large-scale randomized clinical trials to provide a universal policy or standard of care statement. There have been many small studies published that focus on the potential use, efficacy, and safety of regional nerve blocks when compared to traditional parenteral pain medication. These studies provide promising data to encourage further use of this practice and potentially adopt it as a standard of care. However, further investigation is in order, as taking time away from other patients could be disadvantageous if the procedure offers little or no benefit over traditional means of treatment. The following literature review will highlight some of the most prevalent studies in attempt to provide support for the use of regional anesthesia, be it ultrasound guided or not, in the ED for patients with hip fractures.
METHODS
OBJECTIVE. The purpose of this literature review is to decipher the efficacy and safety of pain control provided by regional anesthesia in adults with hip fractures, as compared to traditional parenteral pain medication. Select articles will be utilized to evaluate the theory that patients who receive regional anesthesia in the ED will require less parenteral pain medication and have fewer adverse effects during their hospital stay. The outcome of this evidence-based overview will attempt to provide a summary and recommendation for the clinical utility of regional anesthesia in the ED for hip fractures.
PARTICIPANTS. All studies included in this literature review had a study population of adults over the age of 18. The average age of the populations in the selected studies ranged from 75 to 85 years old, with an overall average of 79. All participants were patients who presented to the ED with a hip fracture, and received either parenteral pain medications, a regional nerve block, or combination of both. In all the selected studies, patients with hip fractures who received regional nerve blocks in the ED were used as independent variables and were compared to a control group of patients who received only standard parental pain control. The dependent variables were defined as the overall amount of parenteral pain medication and overall adverse effects, as specifically defined in each study, noted during the hospital stay.
DATA ACQUISITION. Articles for review were collected using a systematic approach with a designated search engine, specific search terms, and a screening process to help ensure reliability and relevance of articles. The Oklahoma State University Center for Health Sciences Medical Library website provides access to primary literature databases such as PubMed, Embase, Scopus, SciVal, and many others. This was used for primary data collection, as this search engine provided access to a broad range of peer reviewed articles, journals, and databases.8 The following terms were entered to locate potential articles for review: hip fractures, regional nerve blocks, emergency department, ultrasound guided regional nerve blocks, emergency department hip fractures, emergency department regional nerve blocks. A secondary method of search was performed using the obtained articles. Reviewing and investigating the various articles' cited references provided a reliable avenue for locating further literature related to the desired topic. Once articles were deemed to be potentially useful for review, inclusion and exclusion criteria were applied to help ensure relevance and reliability. The inclusion and exclusion criteria are provided in table 1.
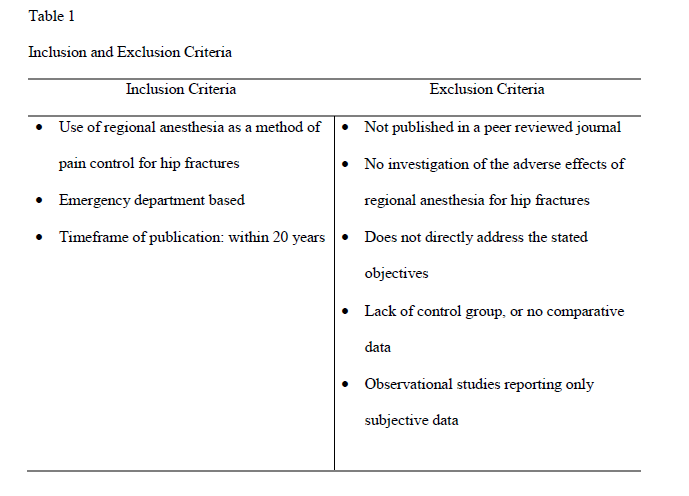
The inclusion criteria were chosen to identify articles that would directly address the proposed theory. The timeframe of the study was deemed important because of the vast advancements in ultrasound technology over the recent past. Adding data from studies using ultrasound served as an important means of making up-to-date clinical recommendations. The exclusion criteria eliminated studies which lacked a control group and comparative data. This criterion was chosen to avoid the risk of observer bias compromising the legitimacy of results. Since there was not a breadth of research on this topic, there were no further stringent exclusion criteria relating to study size, methodology, or statistical data collection. If an article fulfilled all the criteria listed above, it was included in the literature review.
Interpretation of Data. Each article was critiqued by the two main authors of this literature review. Articles were evaluated for their population size, demographics, study location, and timeframe. The investigation of these study characteristics provided evidence for their clinical applicability, generalizability, and external validity. The primary, secondary, and observed outcomes were also evaluated. Importance was placed on ensuring that authors initially stated their primary and secondary outcomes, as opposed to making conclusions at the end of their study. This was necessary to ensure that cofounding variables were not influencing data and data was not altered following results. Again, statistical methodology was not heavily scrutinized, as none of the reviewed studies represented large scale clinical trials. Instead, the basic study approach and resulting data was summarized. The summary of this information provided a basis for the overall strengths and weaknesses of the study and the potential impacts of those factors on data results.
RESULTS
LITERATURE REVIEW: STUDIES WITH ULTRASOUND GUIDANCE. Beaudoin et al1 conducted a randomized controlled trial that compared ultrasound guided femoral nerve blocks to parenteral opioids alone for analgesia in patients with hip fractures. In this study, they did find a statistically significant overall pain reduction in patients who received regional nerve blocks. They also found that patients who only received parenteral opioid medications did not achieve a clinically significant reduction in pain throughout the study. Although this study was not powered to detect statistically significant differences in adverse effects, it may be notable that the regional nerve block group did have a lower overall length of ED stay, less respiratory depression, and less use of rescue opioids. There were some obvious limitations of this study, as it was a small study with only thirty-six patients. Furthermore, there was no established protocol for parental pain control with opioids. Titration was dependent on the treating physician, therefore potentially allowing patients in the two study arms to receive different levels of pain medication titration and administration. Additionally, even though the study was blinded, it is mentionable that the arm receiving the placebo injection actually received a much smaller injection amount, thus potentially unblinding the grouping of the patient to the treating physician. Strengths of this study were that both groups were similar in terms of age, sex, fracture patterns, and initial pain levels. Both groups were randomly assigned, and the study was blinded to the patients. Additionally, the study took place at a large urban ED in the United States (U.S.).
Morrison et al7 conducted a multicenter, randomized controlled trial that took place in three urban ED's in New York. In this study the researchers evaluated the efficacy of ultrasound guided femoral nerve blocks, followed by a continuous fascia-iliaca block. This group was compared to another group who received traditional parenteral analgesia. The randomized groups had no statistically significant differences in patient characteristics. Interviewers and investigators were blinded to the patient's assignment groups, but treating physicians were not. The control group did not receive placebo injections, due to this being deemed unethical. Results of this study indicated that pain levels were significantly less in the intervention group at 1 and 2 hours after ED admission (NRS 4 vs. 8). Pain was assessed on post-operative day 3, which was also less in the intervention group. More interestingly, patients had significantly less pain at rest, during transfers, and while walking in the intervention group. The focus on these specific outcomes gives strength to this study, as these are all clinically relevant assessments. This study also provided information regarding adverse effects. The intervention group required 33% less parenteral opioids for breakthrough pain and adverse effects were significantly lower in the intervention group. Limitations of this study were that patients and treating physicians were not blinded to the study group they were in and total enrollment in this study was fairly low at 153 participants.
Ketelaars et al5 performed a study using ultrasound guided nerve blocks, which focused specifically on the effectiveness and safety of the blocks when performed by ED physicians. This was a prospective, observational study which included sixty-four patients who received femoral nerve blocks, under ultrasound guidance, administered by trained emergency physicians. In this study, they concluded that the ultrasound-guided femoral nerve blocks were an effective and safe modality for pain control in the ED. Their results indicated that patients had a statistically significant reduction in pain, with 69% of patients having reduction at 30 minutes and 83.3% at 60 minutes. Furthermore, no adverse events were reported. Limitations of the study were that it was a prospective observational study, thus there was no blinding of patients or physicians, nor was there a comparison group. Furthermore, some may question the external validity because the physicians were trained by skilled anesthesiologists prior to performing the blocks. Although physicians in this study reported the nerve blocks to be an arbitrary eight out of ten on an ease of use scale, expert training prior to this procedure is not commonplace in every ED. However, considering the limitations, this study did produce overall positive results for pain control and safety and results were comparable to that of Beaudoin.1
LITERATURE REVIEW: STUDIES WITHOUT ULTRASOUND GUIDANCE. Monzon et al6 performed a prospective randomized double-blind study on the effectiveness for fascia-iliaca regional anesthesia in comparison to systemic non-steroidal anti-inflammatory drugs (NSAIDs). In this study, ultimately 154 patients were randomized to either receive a fascia-iliaca nerve block with bupivicane along with 5% dextrose through an intravenous (IV) catheter or a placebo facia-iliaca block with saline injection along with IV NSAIDs. Pain levels were assessed over an eight-hour period. Groups were noted to have no statistical difference in demographics. Data from this study concluded that pain was better controlled in the regional block group at 15 minutes. Pain control was similar at the two and eight-hour mark. The authors did mention that pain ratings at the eight-hour mark were higher, although not statistically higher in the fascia-iliaca group, thus possibly indicating the block wearing off. No rescue opioids were given, indicating the efficacy of both modalities. However, adverse events were significantly lower in the regional nerve block group, denoting the safety profile for regional blocks without the use of ultrasound guidance. This is the only study in this review that used medications other than parenteral opioids for pain relief. This is an important factor, as many countries outside the U.S. do not use opioids as first line for pain control. Similarly, NSAIDs are well known for the gastrointestinal and cardiovascular effects, therefore potentially representing adverse effects not seen in other studies.
A prospective, randomized controlled trial with blinded assessors was authored by Fletcher et al.3 This study evaluated the efficacy of the 3-in-1 nerve block technique. This technique was chosen as it is commonly performed following hip surgery, but it is usually performed by anesthesiologists rather than ED physicians. Thus, there is limited literature to support its use in the ED setting. In this study, patients were assigned to groups either receiving 3-in-1 blocks, along with parenteral opioids, or parenteral opioids alone. They did not receive a placebo injection like some of the previous studies, as their ethics committee considered this unethical. Arguably, the most important aspect they evaluated was specifically pain with movement. In many fracture cases, pain is minimal at rest, but significant with movement. This endpoint is clinically relevant, as pain control while patients are being moved for imaging studies, bed transfers, and physical evaluations is a significant challenge. The data from this study indicates that the patients who received a 3-in-1 block reported significantly faster analgesia and required less overall parenteral opioids over a 24-hour period. Furthermore, no adverse events were reported in the 3-in-1 block arm. Strengths of this study were that enough patient enrollment was achieved to power the desired outcomes and its resulting data is consistent with that shown in other similar studies. Limitations of this study were that ethical reasons inhibited the blinding of patients to treatment groups. However, this potential bias was attempted to be dissipated as nurses who collected the pain assessment data were blinded to the patient allocations
Ritcey et al9 authored arguably the most robust paper on regional nerve blocks for hip fractures in emergency medicine literature to date. This study was a systematic review that included nine studies, some of which are included above. This systematic review attempted to evaluate the results of pain control with regional nerve blocks when compared to traditional pain management. Their focus was on the overall use of opioid analgesia, as well as adverse effects reported. In eight out of nine studies, regional anesthesia was reported to have an "equal or superior benefit,"9 when compared to traditional pain control. Five out of six studies, that investigated the use of parenteral opioids for traditional pain management, reported a statistically significant reduction in opioids in the groups receiving regional anesthesia. The reported adverse effects were noted to be highly variable, and therefore conclusions were not accepted as generalizable. However, they did report that in all the studies, not one life threatening complication from regional anesthesia occurred. Overall, this systematic review offers support for regional anesthesia as being non inferior, and possibly superior, in reducing pain from hip fractures. Similarly, there is convincing evidence that regional nerve blocks decrease the need for opioids.
DISCUSSION
From the literature, we have gained insight that regional anesthesia can offer a more rapid, efficacious, and safe alternative to pain control in patients with hip fractures when compared to traditional opioids, NSAIDs, and other modalities of pain control. Although the composition of data is based on many small studies, at moderate risk for bias, there seems to be a common theme of positive results reproduced by nearly every study. Generalizability and reproducibility speak volumes towards the legitimacy of data when it comes to medical research. Therefore, based on the current composition of data, it seems that there is moderate support for the use of regional nerve blocks in the ED, as this may improve many clinically relevant and patient oriented aspects of ED hip fracture care.