Daniel Tritz, OSU Center for Health Sciences, OMS IV
Yoon Cho, D.O., Oklahoma State University Center for Health Sciences, Department of Radiology
Brooke White, D.O., Oklahoma State University Center for Health Sciences, Department of Radiology
Donald von Borstel, D.O. Oklahoma State University Center for Health Sciences, Department of Radiology
Abstract
Mucinous minimal deviation endocervical adenocarcinoma, also known as adenoma malignum, is a rare subtype of mucinous adenocarcinoma of the cervix; adenoma malignum is about 1-3% of endocervical adenocarcinoma. It shows no ethnic predilection and can present in a wide age range with average age being between the 5th and 6th decades of life. It can be associated with Peutz-Jeghers syndrome. Patients often present with watery or mucinous vaginal discharge and/or irregular uterine bleeding. The cervix may be firm on physical exam. Endocervical biopsies can be misleading due to the benign pathologic appearance or may be normal, which may lead to misdiagnosis. The main treatment for this condition is surgical resection.
Introduction
This case study illustrates the atypical clinical presentation, diagnostic evaluation, and therapeutic intervention of a patient with the rare diagnosis of endocervical minimal deviation adenocarcinoma.
Case Report
A 53-year-old female presented with rectal pain on sitting and pelvic discomfort for 2-months prior to her initial evaluation by her primary care physician. She was then referred to a gastroenterologist for colonoscopy. She denied any other gastrointestinal symptoms, nausea, vomiting, blood in her stool, or change in bowel movements at that time. The colonoscopy identified a mass that was 7 cm from the anal verge. Multiple biopsies were performed that identified the mass as adenocarcinoma extending to all margins.
A follow-up computed tomography (CT) scan abdomen and pelvis revealed an additional 6.4cm lesion in the lower uterine segment with poor visualization of the rectal mass (Figure 1). She then received a PET/CT scan which identified hypermetabolic activity in the rectum and the lower uterine segment. The patient had a rectal ultrasound with a magnetic resonance image (MRI) of the abdomen and pelvis for further cancer staging.
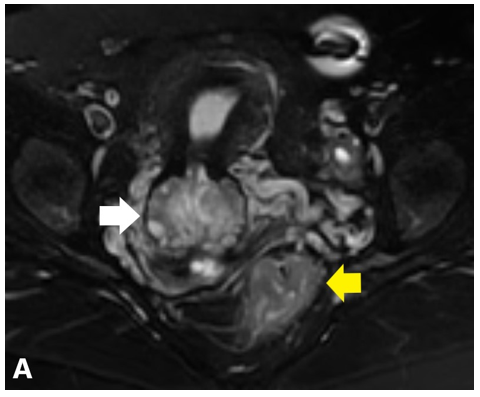
Figure 1. A
Figure 1. B
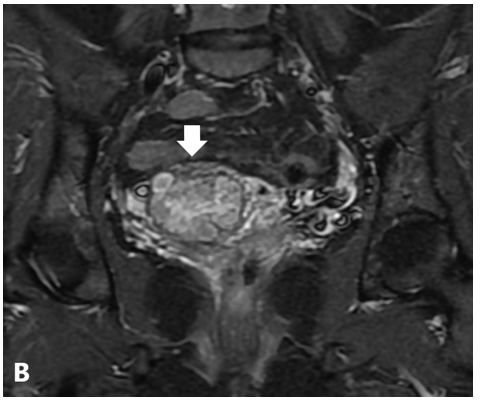
Figure 1. C
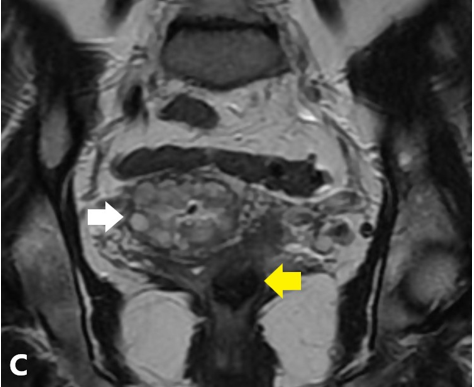
Figure 1A. On a coned down T2-weighted fat saturated axial sequence of the pelvis, the cervix demonstrates numerous hyperintense cystic lesions within an enlarged cervix (solid white arrow). There is also a hypointense mass seen at the sigmoid colon (solid yellow arrow). B. On coronal STIR sequence of the pelvis, the cystic lesions demonstrates hyperintense signals with enlargement of the cervix. The cysts are seen extending deep into the cervical stroma with an associated solid component. C. Coronal T2-weighted fast relaxation fast spin echo sequence (FRFSE) sequence demonstrates mixed solid and cystic cervical lesion (solid white arrow).
Figure 3.
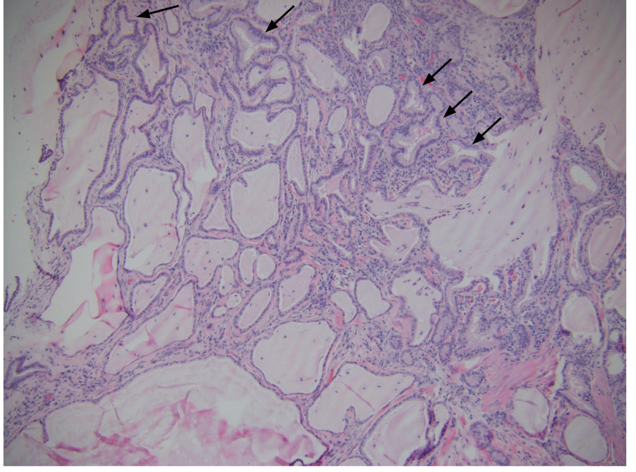
Figure 3. Numerous mucin-producing architecturally abnormal glands (black arrows) lined by cuboidal to columnar cells with minimal cytologic atypia with basally located nuclei.
Discussion
It is estimated that almost 300,000 women in the US were living with cervical cancer in 2016 1. Squamous cell carcinoma is responsible for about 80% of cervical cancer with adenocarcinoma representing the other 20%2. Minimal deviation adenocarcinoma, or adenoma malignum, is a subtype of cervical cancer which is caused by proliferation of well-differentiated gastric mucinous cells3. Common presenting symptoms for this rare type of cancer include profuse mucoid vaginal discharge and irregular or post-coital vaginal bleeding4,5. In comparison, our patient denied any significant symptoms and only complained of vague rectal and vaginal discomfort with sitting.
Since squamous cell carcinoma is a more common type of cervical cancer, there has been a higher rate of success at preventing squamous cell carcinoma, which has a near 100% link to human papilloma virus (HPV), with preventative medical options such as HPV vaccines 6. Unfortunately, adenoma malignum, or minimal deviation adenocarcinoma, is not related to HPV and shows association with other systemic conditions such as Peutz-jegher syndrome and Lynch syndrome. The incidence of this condition has not decreased at the same rate compared to squamous cell carcinoma7,8,9.
The main differential diagnosis for adenoma malignum would be a conglomerate of nabothian cysts or endocervical glandular hyperplasia. Sonographic imaging findings of adenoma malignum consists of cystic lesions seen in the lower uterine segment with enlarged cervix. MRI shows multiple irregular T2 hyperintense cystic lesions with enhancing stroma on post-contrast image. Takatsu et. al. described the finding as "Cosmos pattern" as the irregular cystic lesions often seen in floret-like pattern10. The lesions may demonstrate restrictions on diffusion weighted sequence (DWI)3,11. Nabothian cysts can be seen deep within the cervical stroma which can make the diagnosis difficult. The cervix can be enlarged in both etiologies although the main distinguishing factor would be the enhancing solid component of adenoma malignum which would not be present with nabothian cysts. Nabothian cysts also are typically smaller and demonstrate well-defined margins which would help differentiate them12. An additional entity in the differential diagnosis is endocervical glandular hyperplasia which is thickening of the endocervical mucosa with resultant cyst formation in the endocervix. Endocervical hyperplasia is typically hyperintense on T1- and T2-sequences. A differentiating feature of hyperplasia is the lack of an enhancing solid component that is commonly seen with adenoma malignum. Ultrasound may be the initial imaging to use in patients that have an unconfirmed genitourinary malignancy, but MRI is more specific and better for staging as there is a higher resolution for soft tissues13. Bourgioti et. al. quantified the ability of MRI to accurately stage cervical cancer compared to clinical assessment and found that MRI was superior in comparison to clinical assessment alone, and even better results when MRI and clinical assessment were combined14.
The European Society for Medical Oncology suggests different treatment approaches depending on the staging and metastatic status of cervical cancer, but does not differentiate between adenocarcinomas and squamous cell histology15. Treatment of earlier stage disease requires local surgery with recommended neoadjuvant chemotherapy to reduce tumor size, eradicate micrometastatic disease, and increase tumor vascularization to reduce the number of hypoxic cells. In advanced or metastatic cases, such as ours, current treatment recommendations are more extensive including surgery (radical hysterectomy with bilateral salpingo-oophorectomy with possible lymph node dissection), three-drug chemotherapy, and potential radiation for better outcomes15,16. Unfortunately, adenocarcinoma of the cervix is less responsive to chemoradiotherapy than squamous cell carcinoma and often results in decreased overall survival at 10-year follow-up17.
Poor prognosis for adenoma malignum commonly occurs from delays in diagnosis due to benign symptoms and benign appearing endocervical biopsy causing late presentation3. Cervical adenocarcinoma, as a whole, has a poor response to radiation and chemotherapy with treatment being less successful than squamous cell. Poor response to radiation is surprising given that adenocarcinomas of the cervix are most often well-differentiated and stage I or II when first diagnosed18. Adenoma malignum has few studies looking at the poor prognosis separate from other cervical adenocarcinomas, and is thus discussed in general terms applicable to both3.The most common recommendation for the prevention of all forms of cervical cancer is HPV vaccination19. Since HPV has been associated with the majority of cervical cancer, the current recommendation by CDC for HPV vaccination is to initiate routine vaccination at age of 11-12 years or to vaccinate females aged 13-26 years if they have not adequately vaccinated previously20.
Screening for cervical cancer, including pap smears and HPV serology, has improved the detection of asymptomatic early cellular metaplasia. Our patient had no documentation of being diagnosed with HPV or being vaccinated for it. Unfortunately, as mentioned above, adenoma malignum has not been closely associated with patients infected with HPV21,22. Screening tools to aid in the diagnosis of adenoma malignum are the HIK1083-latex agglutination test or MUC6 that identifies gastrin mucus present in cervical discharge23-25. With all of the screening techniques, any positive or unspecified results warrant radiographic follow-up with ultrasound and biopsy sampling followed by MRI.
Our case describes a rare case of mucinous minimal deviation endocervical adenocarcinoma, also known as adenoma malignum, with concurrent occurrence of an independent colonic adenocarcinoma. Our patient was further complicated by having an atypical clinical presentation with no substantial genitourinary or gastric symptoms, which may have led to a delay in diagnosis. Imaging work up with ultrasound and staging by MRI played an integral role in diagnosis of our patient and allowed for expedited surgical management before further complications or distant metastasis could occur.
Statement of funding sources:
No funding was obtained for the writing of this manuscript.
Conflicts of interest disclosures:
None of the authors have conflicts of interest or relevant financial relationships to disclose.
Key Words: Adenocarcinoma, Uterine mass, Adenoma malignum
References
1. Cancer of the Cervix Uteri - Cancer Stat Facts. SEER. https://seer.cancer.gov/statfacts/html/cervix.html. Accessed August 1, 2019.
2. Cancer TIC of ES of C, The International Collaboration of Epidemiological Studies of Cervical Cancer. Comparison of risk factors for invasive squamous cell carcinoma and adenocarcinoma of the cervix: Collaborative reanalysis of individual data on 8,097 women with squamous cell carcinoma and 1,374 women with adenocarcinoma from 12 epidemiological studies. International Journal of Cancer. 2007;120(4):885-891. doi:10.1002/ijc.22357
3. Talia KL, McCluggage WG. The developing spectrum of gastric-type cervical glandular lesions. Pathology. 2018;50(2):122-133.
4. Lim K-T, Lee I-H, Kim T-J, Kwon Y-S, Jeong J-G, Shin S-J. Adenoma malignum of the uterine cervix: Clinicopathologic analysis of 18 cases. Kaohsiung J Med Sci. 2012;28(3):161-164.
5. Toki T, Zhai YL, Park JS, Fujii S. Infrequent occurrence of high-risk human papillomavirus and of p53 mutation in minimal deviation adenocarcinoma of the cervix. Int J Gynecol Pathol. 1999;18(3):215-219.
6. Goodman A. HPV testing as a screen for cervical cancer. BMJ. 2015;350:h2372.
7. Ferguson AW, Svoboda-Newman SM, Frank TS. Analysis of human papillomavirus infection and molecular alterations in adenocarcinoma of the cervix. Mod Pathol. 1998;11(1):11-18.
8. Pirog EC. Diagnosis of HPV-negative, gastric-type adenocarcinoma of the endocervix. Methods Mol Biol. 2015;1249:213-219.
9. McGowan L, Young RH, Scully RE. Peutz-Jeghers syndrome with "adenoma malignum" of the cervix: A report of two cases. Gynecol Oncol. 1980;10(2):125-133.
10. Takatsu A, Shiozawa T, Miyamoto T, et al. Preoperative differential diagnosis of minimal deviation adenocarcinoma and lobular endocervical glandular hyperplasia of the uterine cervix: a multicenter study of clinicopathology and magnetic resonance imaging findings. Int J Gynecol Cancer. 2011;21(7):1287-1296.
11. Park KJ, Kim M-H, Kim JK, Cho K-S. Gastric-Type Adenocarcinoma of the Uterine Cervix: Magnetic Resonance Imaging Features, Clinical Outcomes, and Prognostic Factors. Int J Gynecol Cancer. 2018;28(6):1203-1210.
12. Yamashita Y, Takahashi M, Katabuchi H, Fukumatsu Y, Miyazaki K, Okamura H. Adenoma malignum: MR appearances mimicking nabothian cysts. AJR Am J Roentgenol. 1994;162(3):649-650.
13. Small W Jr, Bacon MA, Bajaj A, et al. Cervical cancer: A global health crisis. Cancer. 2017;123(13):2404-2412.
14. Bourgioti C, Chatoupis K, Rodolakis A, et al. Incremental prognostic value of MRI in the staging of early cervical cancer: a prospective study and review of the literature. Clin Imaging. 2016;40(1):72-78.
15. Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2017;28(suppl_4):iv72-iv83. doi:10.1093/annonc/mdx220
16. Couvreur K, Naert E, De Jaeghere E, et al. Neo-adjuvant treatment of adenocarcinoma and squamous cell carcinoma of the cervix results in significantly different pathological complete response rates. BMC Cancer. 2018;18(1):1101.
17. Kaidar-Person O, Yosefia S, Abdah-Bortnyak R. Response of adenocarcinoma of the uterine cervix to chemoradiotherapy. Oncol Lett. 2015;9(6):2791-2794.
18. Zhou J, Wu S-G, Sun J-Y, et al. Comparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysis. Journal of Cancer Research and Clinical Oncology. 2017;143(1):115-122. doi:10.1007/s00432-016-2246-9
19. Petrosky E, Bocchini JA Jr, Hariri S, et al. Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2015;64(11):300-304.
20. HPV | For Clinicians | Vaccination Schedules and Recommendations | CDC. August 2019.
21. Xu J-Y, Hashi A, Kondo T, et al. Absence of human papillomavirus infection in minimal deviation adenocarcinoma and lobular endocervical glandular hyperplasia. Int J Gynecol Pathol. 2005;24(3):296-302.
22. Odashiro AN, Odashiro DN, Nguyen G-K. Minimal deviation endometrioid adenocarcinoma of the cervix: report of three cases with exfoliative cytology. Diagn Cytopathol. 2006;34(2):119-123.
23. Omori M, Hashi A, Ishii Y, et al. Clinical impact of preoperative screening for gastric mucin secretion in cervical discharge by HIK1083-labeled latex agglutination test. Am J Clin Pathol. 2008;130(4):585-594.
24. Ishii K, Hosaka N, Toki T, et al. A new view of the so-called adenoma malignum of the uterine cervix. Virchows Arch. 1998;432(4):315-322.
25. Wada T, Ohishi Y, Kaku T, et al. Endocervical Adenocarcinoma With Morphologic Features of Both Usual and Gastric Types. The American Journal of Surgical Pathology. 2017;41(5):696-705. doi:10.1097/pas.0000000000000833
26. Takatsu, A. et al. Preoperative differential diagnosis of minimal deviation adenocarcinoma and lobular endocervical glandular hyperplasia of the uterine cervix: a multicenter study of clinicopathology and magnetic resonance imaging findings. Int. J. Gynecol. Cancer 21, 1287-1296 (2011).