A Rare Case of anomalous third coronary artery and multiple coronary artery fistulae
Khizer A. Sikander, DO,
Stephen B. Dixon, DO,
Steve Kim, DO.
ABSTRACT
We present an extremely rare case of a patient who during cardiac catheterization was found to have multiple coronary artery fistulae including a third coronary artery. In our case the patient was diagnosed in the seventh decade of life and due to minimal clinical symptoms did not require further intervention. The case presents a rare combination of an anomalous coronary artery and multiple coronary artery fistulae.
INTRODUCTION
Coronary artery fistula is usually identified incidentally during coronary angiography in 0.1% to 0.2%7 of patients with the majority of cases involving a single coronary artery. Furthermore, anomalous coronary arteries are also a rare finding reported in 0.2% to 1.3%9 of adult patients undergoing coronary angiography. We present an extremely rare case of a patient, who on cardiac catheterization was found to have multiple coronary artery fistulae including a third coronary artery.
CASE PRESENTATION
A 72-year-old Caucasian male presented to the clinic with a chief complaint of shortness of breath and aching right-sided chest pain of two weeks duration. Past medical history included hypertension and hyperlipidemia. He was seen at an urgent care and subsequently underwent a
treadmill exercise stress test, which showed ST segment depression in the inferior leads. Given the findings on stress test and his risk factors for coronary artery disease he was referred to outpatient cardiology clinic for further evaluation. Options for further evaluation were discussed with the patient and he elected to proceed with coronary CT angiogram. The coronary CT angiogram was unable to be completed due to significant elevated coronary artery calcium score of 1341.
He was seen for a follow-up visit one month later. At that point, the patient stated his shortness of breath had resolved, but he was still having vague aching right-sided chest pain. On physical exam, his vitals were BP 168/69 left arm supine, Pulse 75, RR 16. Normal JVD of <6 cm H2O, no peripheral edema, normal S1/S2, no S3 or S4, and a faint continuous murmur heard only in the left second intercostal space. The remainder of the physical exam was unremarkable. The electrocardiogram and chest radiograph were normal. The laboratory findings were within normal limits. In light of persistent chest pain, an abnormal stress test, and elevated coronary artery calcium score, cardiac catheterization was recommended to further delineate his coronary anatomy.
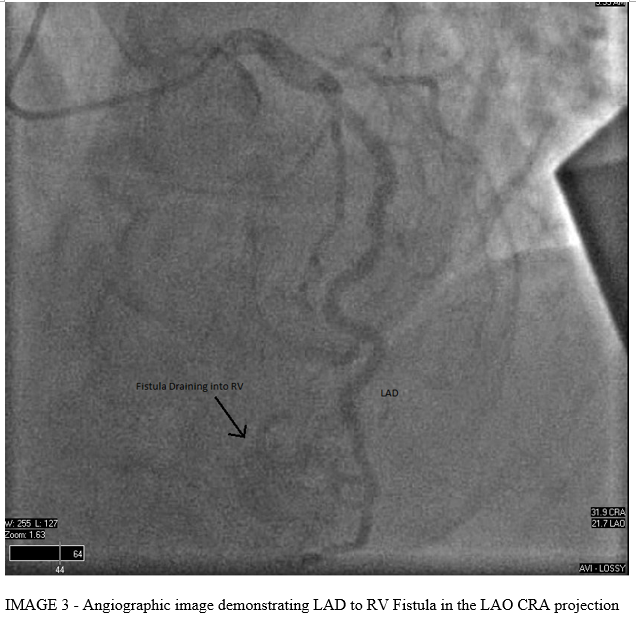
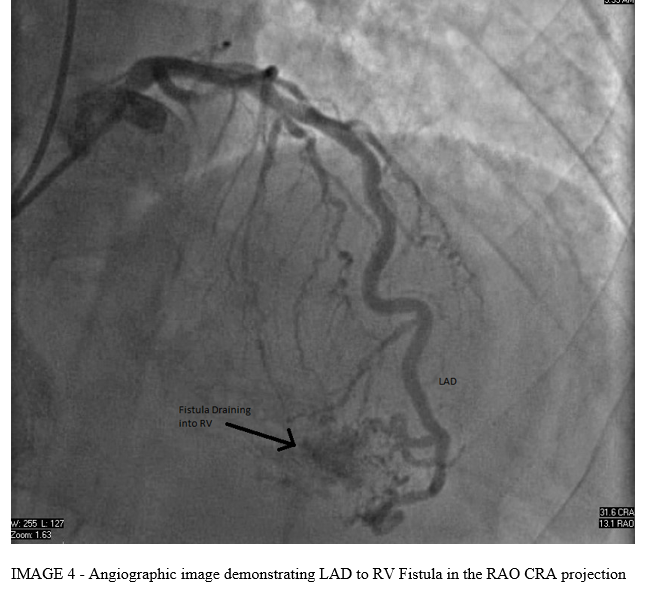
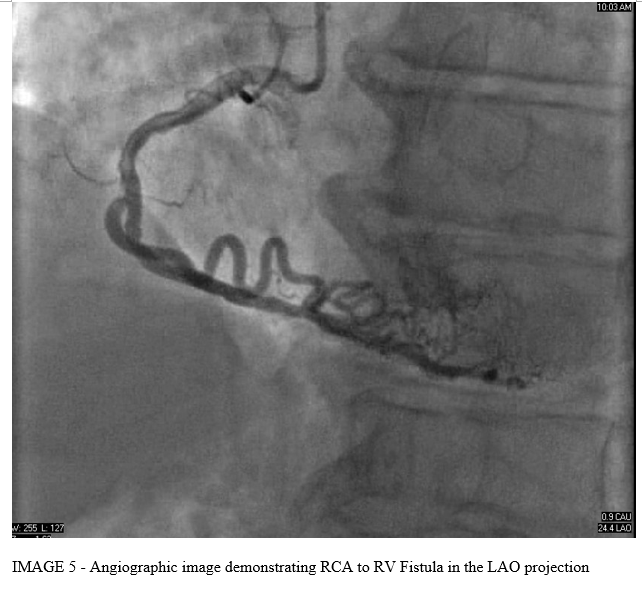
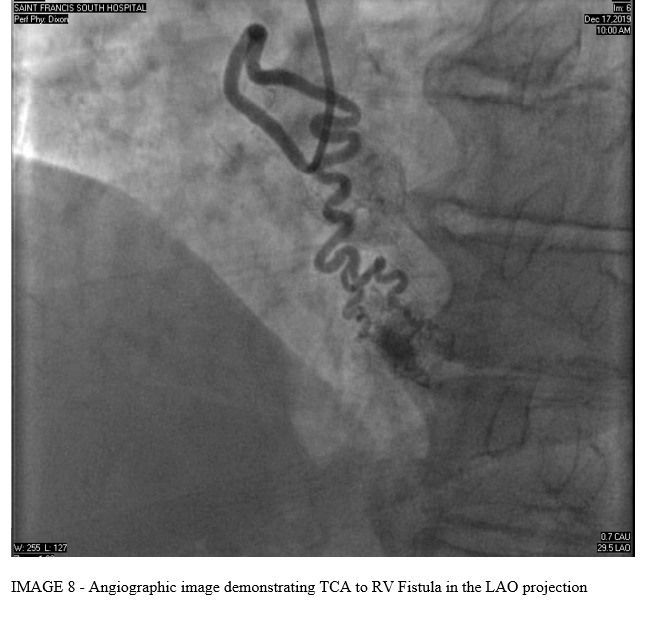
Left Heart catheterization demonstrated a normal left main coronary artery (LMCA), left anterior descending coronary artery (LAD) with mild proximal stenosis, left circumflex coronary artery (LCx) with mild proximal stenosis, right coronary artery (RCA) with mild distal stenosis, and normal third coronary artery (TCA). Incidentally, there were multiple coronary artery to right ventricle (RV) fistulae noted from the left anterior descending, right coronary, and third coronary arteries.
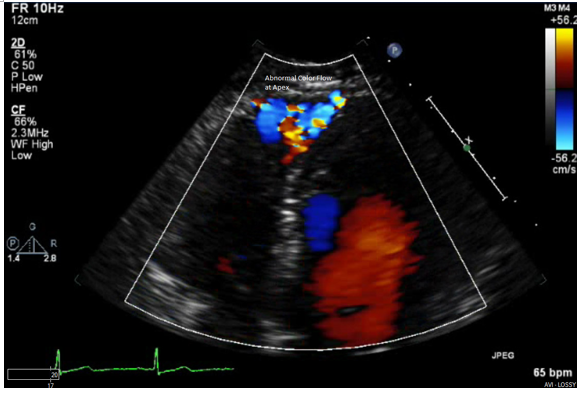
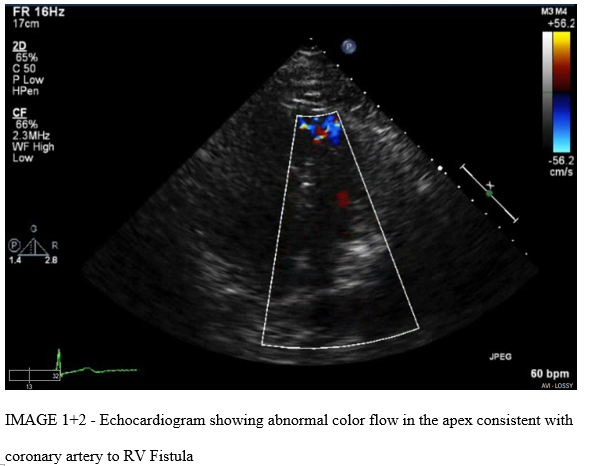
The patient subsequently underwent a two-dimensional echocardiogram, which showed an ejection fraction of 55%, no wall motion abnormalities, normal right ventricle cavity and systolic function. Abnormal color flow Doppler was seen near the apex. Mean pulmonary artery pressures were calculated to be 21 mmHg and the Qp/Qs (Pulmonary-Systemic Shunt Ratio) was calculated to be 1.5.


DISCUSSION
Coronary artery fistula is an anomalous communication between a coronary artery and the cardiac chambers or the great vessels. The majority of these are congenital in origin but some acquired cases have been reported after trauma or cardiac surgery6. They are usually isolated but may be associated with other congenital defects. The incidence of coronary artery fistula is reported to be less than 1% based on several studies7. The majority of these reported cases were of a single coronary artery fistula with very few studies documenting the presence of multiple coronary artery fistulae.
The incidence of anomalous coronary arteries found on angiography has been reported to be between 0.2% to 1.3% in the adult population9. The majority of these cases involve the left anterior descending artery or left circumflex arteries.1 The third coronary artery is described in literature as a separate origin of the conus artery or a right ventricular branch arising from the right aortic cusp.5 Coronary artery fistulae involving the third coronary artery are extremely rare.
The hemodynamic effect of the fistula depends on the site of the drainage and most commonly affects the right side of the heart creating a left to right shunt.3 Patients with this finding are usually asymptomatic at a young age and develop symptoms only in the presence of a large shunt.11,4
Patients usually present with complications related to the coronary artery fistula starting in the third decade of life. These include congestive heart failure, ischemia of the myocardium related to "steal" phenomenon, thrombosis and embolism, arrythmias, and rupture leading to cardiac tamponade.
Diagnosis is usually made incidentally on coronary angiography. Coronary angiography can help characterize the anatomy of the fistula including the location, size, and drainage tract. Other modalities that are helpful in the diagnosis of coronary artery fistulae include transthoracic echocardiogram, transesophageal echocardiogram, multi-detector row computed tomography, and magnetic resonance angiography. 2
Treatment is based on the hemodynamic significance of the fistula along with the patient's age and clinical presentation. Some indications for treatment include significant pulmonary hypertension, large arteriovenous shunt, congestive heart failure, myocardial ischemia, and risk of rupture.10 Treatment options include surgical closure or transcatheter based intervention such as coil embolization or stent occlusion.8
CLINICAL BOTTOM LINE
This is a rare case demonstrating a patient with left anterior descending artery, right coronary artery, and third coronary artery to the right ventricle fistulae diagnosed incidentally in the 7th decade of life. It also demonstrates that despite multiple fistulae, based on minimal clinical symptoms and echocardiographic findings, this is likely a benign finding that does not warrant intervention.
REFERENCES
1. Chen HY. Aberrant origin of the conus branch: Diagnosis of split right coronary artery with two separate ostia by conventional angiography. Exp Clin Cardiol. 2010 Spring; 15(1): 9-10.
2. Sunkara A, Lakshmi HC, Su Min C, Barker C. Coronary Artery Fistula. Methodist Debakey Cardiovasc J. 2017 Apr-Jun; 13(2): 78-80.
3. Sagar D, Hernandez A, Heimowitz T. Coronary Artery-Left Ventricle Fistula: A Case Report of a Rare Connection Error!. Cureus. 2015 Apr; 7(4): e266.
4. Sharma UM, Aslam AF, MD, Tak T. Diagnosis of Coronary Artery Fistulas: Clinical Aspects and Brief Review of the Literature. Int J Angiol. 2013 Sep; 22(3): 189-192.
5. Schlesinger NJ, Paul M, Wessler S. The conus artery: A third coronary artery. American Heart Journal. Volume 38, Issue 6, December 1949, Pages 823-836.
6. Abdelmoneim SS, Mookadam F, Moustafa SE, Holmes DR. Coronary artery fistula with anamolous coronary artery origin: A Case report. JASE. VOLUME 20, ISSUE 3, P333.E1-333.E4, MARCH 01, 2007.
7. Vavuranakis M, Busch CA, Boudoulas H. Coronary artery fistulas in adults: incidence, angiographic characteristics, natural history. Catheter Cardiovasc Diagn. 1995; 35: 116-120.
8. Cascaes DL, Teixeira de Gois A, Hueb W. et al. Large bilateral coronary artery fistula: the choice of clinical treatment. Arq Bras Cardiol. 2009;93(3): e36-e37.
9. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990; 21:28-40.
10. Sherwood MC, Rockenmacher S, Colan SD, Geva T. Prognostic significance of clinically silent coronary artery fistulas. Am J Cardiol 1999;83:407-11.
11. Quershi SA, Orphanet J. Coronary arterial fistulas. Rare Dis. 2006;1:51.