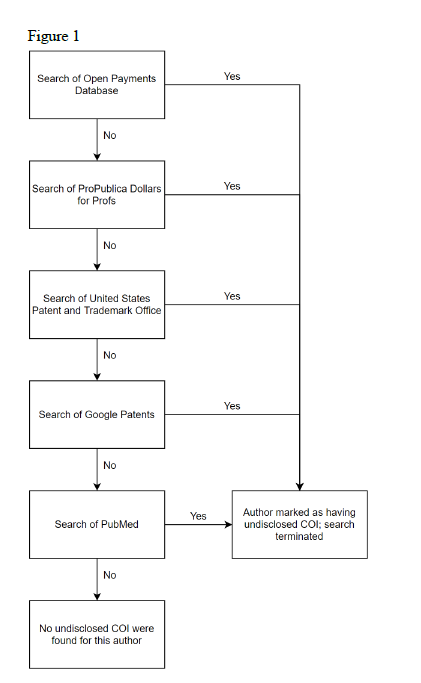
Figure 1. Stepwise search for undisclosed COI among systematic review authors
Risk of bias evaluations
We assessed the risk of funding bias within the systematic reviews using the Cochrane Collaboration’s criteria, which included the following 4 items from Mandrioli et al19: (1) whether replicable and “well-defined” criteria for study inclusion/exclusion were used; (2) whether multiple assessors took part in selecting studies for inclusion/exclusion; (3) whether authors used a comprehensive search strategy; and (4) whether potential sources of bias were controlled for in the primary studies included in the review. Investigators assigned a yes, no, or unclear response to each of the inquiries. Overall risk of bias was considered low if 3 or more of the aforementioned criteria were met. If not, we considered the systematic review to have a high risk of bias.
Statistical Analysis
When necessary, the results were quantified using illustrative statistics and analyzed with Fisher’s exact tests. Fisher’s exact tests were used to compare the presence of relationships between industry and authors of systematic reviews. Stata 16.1 (StataCorp, LLC, College Station, TX) was used for all analyses.
Results:
Our search provided 505 potential records. Following removal of duplicates and other ineligible studies based on title and abstract screening, 107 studies were included for full-text review. Following full-text screening, 17 systematic reviews regarding proximal humerus fracture treatment were included for data extraction. (Figure 2)
Systematic Review Characteristics
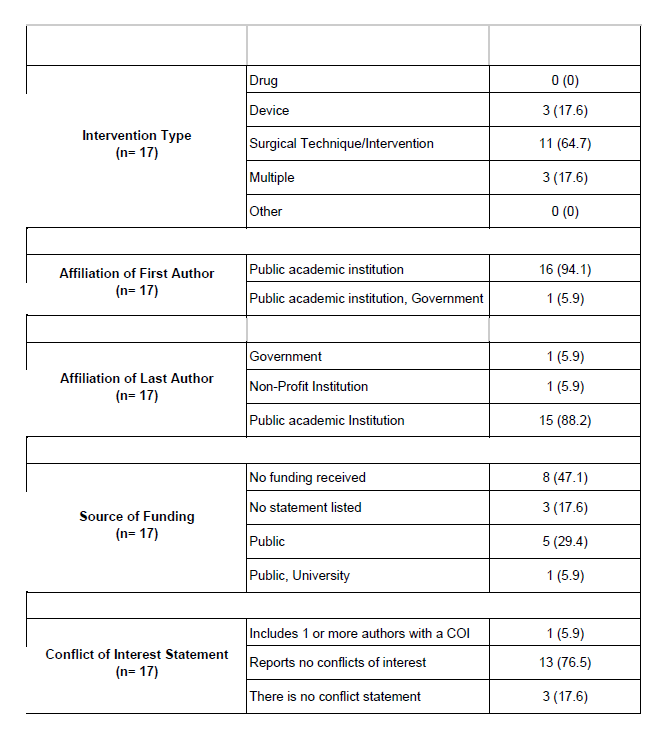
Our study included 17 systematic reviews and meta-analyses conducted by 93 authors and published within 16 journals. The most common journal represented in our sample was Orthopaedics & traumatology: Surgery and Research (2; 11.8%). Most systematic reviews (11/17; 64.7%) evaluated surgical techniques or interventions and the most common source of sponsorship was public funding (5/17; 29.4%). (Table 2) Of the 17 systematic reviews, 7 (41.2%) had at least one author with a COI. (Table 3)
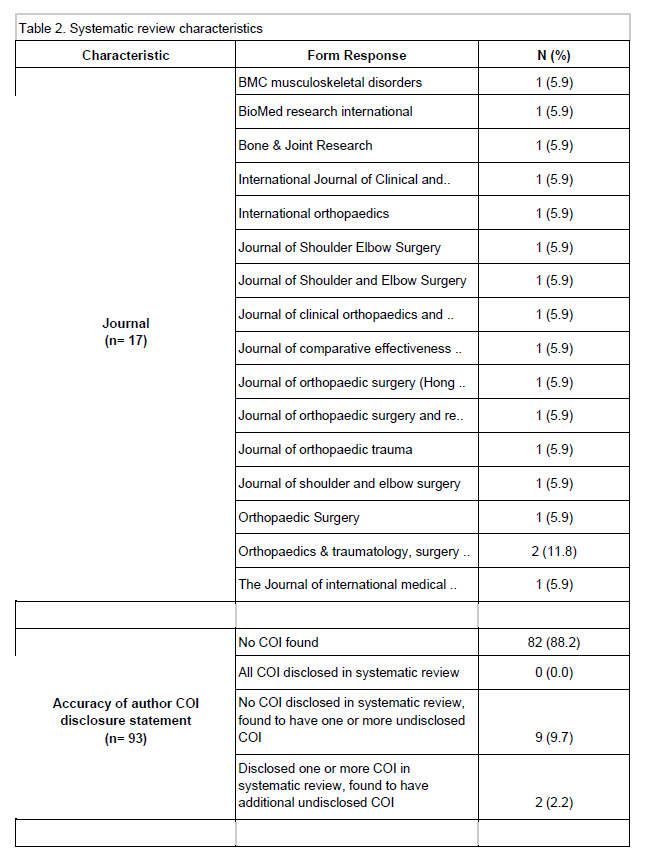
Author Characteristics
Of the 93 review authors, 11 (11.8%) were found to have some form of COI. Of these 11 authors, none completely disclosed all COI within the systematic review, 2 (2.2%) disclosed one or more COI but were found to have an additional undisclosed COI, and 9 (9.7%) were found to have only undisclosed COI. Additional author and study characteristics are provided in Table 2.
Relationship between COI and favorability of results and conclusions
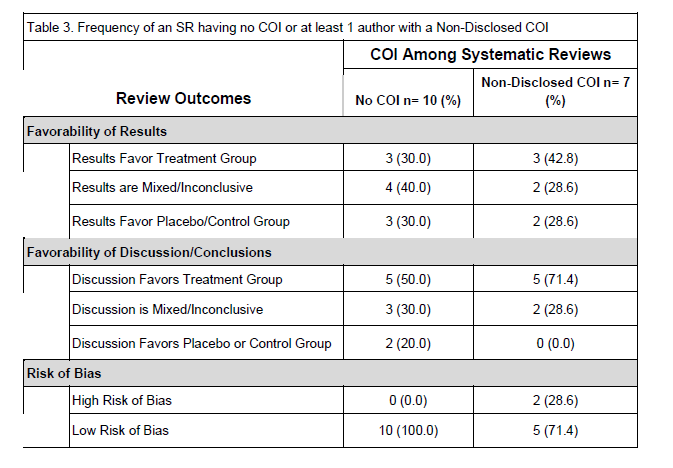
Of the 7 systematic reviews with non-disclosed COIs, 3 (42.8%) reported narrative results in favor of the treatment group. Additionally, 5 (71.4%) reported discussions/conclusions favoring the treatment group. With respect to the 10 systematic reviews with no conflicted authors, 3 (30.0%) reported results favoring the treatment group and 5 (50.0%) reported discussions/conclusions favoring the treatment group. (Table 3) Fisher’s exact did not show a statistically significant association between COI and favorability of results and conclusions.
Relationship between sponsorship and favorability of results and conclusions
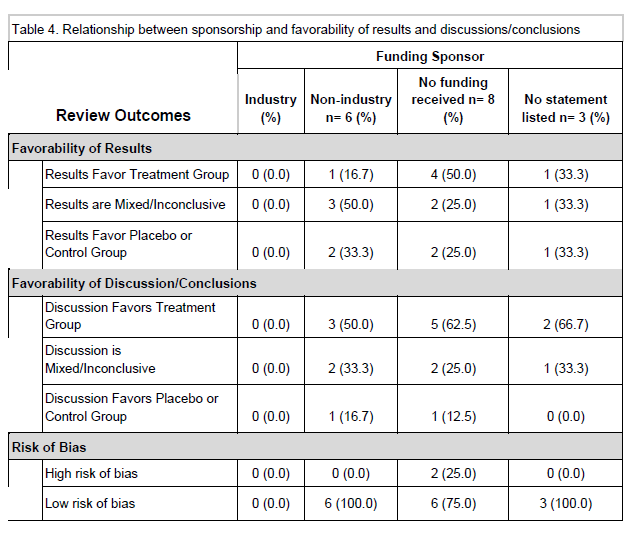
Six systematic reviews (of 17; 35.3%) received external sponsorship, 8 (of 17; 47.1%) did not receive external sponsorship, and 3 (of 17; 17.6%) did not disclose whether the review was supported by an external sponsor. No significant relationship between favorability of the results or discussion/conclusions and article sponsorship was found. Considering none of the systematic reviews in our sample were industry-sponsored, we were unable to assess if a relationship exists between industry vs non-industry-sponsorship and outcomes of systematic reviews. (Table 4).
Relationship between risk of bias and industry sponsorship and conflicts of interest
None of the systematic reviews were funded by industry, thus an association between industry sponsorship and risk of bias was not assessed for. Of the systematic reviews with no COI among authors, none (0%) were considered to have high risk of bias. In contrast, 2 systematic reviews (of 7; 28.6%) with at least one conflicted author were found to have a high risk of bias. (Table 3) Due to low sample size, no statistically significant association between COI and review outcomes was detected.
Discussion:
Approximately two out of five systematic reviews regarding the treatment of proximal humerus fractures had at least one author with an undisclosed COI. Despite high rates of nondisclosure, we found no significant association between the presence of author COI––either disclosed or undisclosed––with the favorability of systematic review results and conclusions. Due to a lack of industry-funded systematic reviews in our sample, we were unable to ascertain whether industry-sponsorship increased the likelihood of reporting favorable results and conclusions.
Author COI, whether disclosed or undisclosed, carries the potential to introduce bias into the medical literature. For example, Okike et al. found podium presentations at conferences within the field of orthopedic surgery were more likely to present positive findings when individuals had conflicts of interest related to royalties, stock options, and consultant or employee status.20 Narain et al. also found that orthopedic research articles on cervical disc arthroplasty more often presented positive outcomes when conflicts of interest were present.21 Kjaergaard and Als-Nielson found that RCTs were more likely to reach significant results favoring the experimental group when financial competing interests were declared.22 In our sample, a similar association between author COI and the favorability of results and conclusions was not identified; however, our findings suggest the completeness of author COI disclosure is low and poses as an actionable item by which research stakeholders may improve upon in order to better the quality of research and public trust in research outcomes.
The main funding sponsors in the systematic reviews studied included public grants and university funding. A disconnect from industry alludes to the lower likelihood that these systematic reviews contain inherent bias.23,24 Although it is suggested that industry plays a crucial role in furthering orthopedic research,25 industry funding is still vulnerable to a variety of biases, such as intentionally or unintentionally searching for data significance. Previous studies have shown that industry sponsorship is associated with an increased likelihood of positive outcome reporting.23,24 For example, a 2017 Cochrane review found industry sponsorship was associated with increased likelihood of reporting efficacious results and conclusions demonstrating favorability towards a sponsor’s drug or device despite similar harm results when compared to non-industry sponsored drug and device studies.26 In the same review, drug and device industry-sponsored studies had higher rates of discordance between results and conclusions than in non-industry sponsored studies. Another study found that 85% of orthopedic clinical trials reporting industry funding reported favorable outcomes to the novel treatment.27 Given the lack of industry sponsored studies in our sample, a clinically significant association between study sponsorship and favorability of results and conclusions could not be identified. Despite the implications of industry-funded studies, Hozack et al. argued that the connections made by physician-scientists could bring ample opportunity for research output by the individual or institute.28 Nevertheless, Friedberg et al. reported, within the field of oncology, industry funding was significantly associated with studies yielding negative results going unpublished. While more funding could increase research output, ensuring that all data are published and readily available is of great importance. Unpublished negative results, in the industry's favor, can allude to a rise in unreliable overall results within systematic reviews.29,30
Recommendations
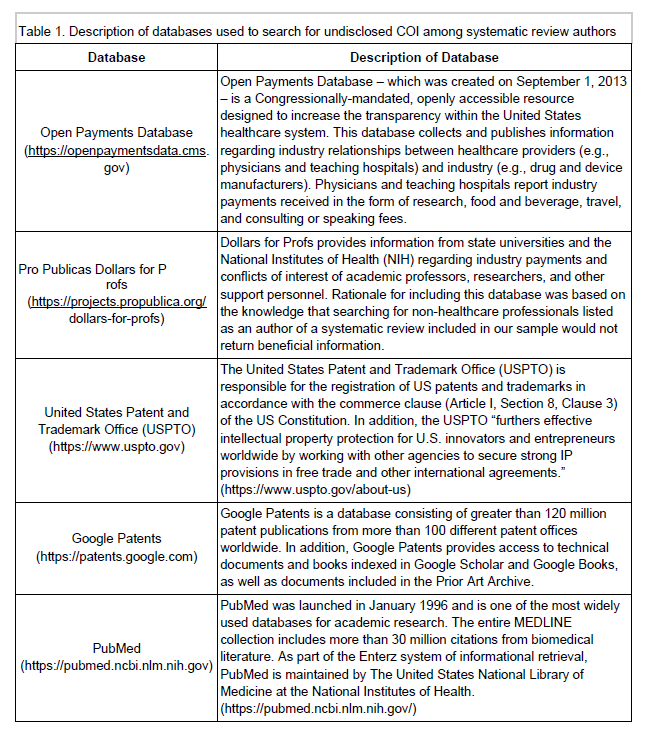
COIs may lead to alterations in the data presented by authors. Open Payments Database and Dollars for Profs are beneficial tools that may help patients, colleagues, and researchers distinguish reliability of medical professionals within the United States (US). Although our study did not find significant evidence of skewed results within our included papers due to COIs, the lack of awareness leaves proximal humerus fracture studies vulnerable to potential bias in the future. Journals should compare and align authors with databases such as Open Payments Database and Dollars for Professors to make sure that disclosures are being addressed in articles. There were also certain articles that had no comments on disclosures for COIs, therefore there should be a strong emphasis to require that all published literature have a disclosed COIs section. Additionally, a large portion of authors in our study had international affiliations with countries including China, the United Kingdom, Sweden and the Netherlands, and they were not found on either OpenPayments Database or Dollars for Profs. If a universal database were to be made accessible, the process of locating an author’s COIs would be less challenging.
Strengths and Limitations
As for our strengths, all authors completed training prior to commencement of data extraction. Completion of calibration exercises amongst data extractors increased the inter-rater reliability between respondents. In addition, data was extracted in a masked, triplicate fashion, ensuring accurate information was collected. Finally, our protocol – which was developed a priori – and study materials have been provided on a public repository, thus increasing the transparency and reproducibility of our results. As for our limitations, Open Payments Database and Dollars for Professors restricted our search to only the U.S.-affiliated authors. Moreover, this study was cross-sectional in design and was limited to studies published between September 2016 and June 2020. Use of a different date range may result in differing outcomes. Lastly, our study was specific to literature pertaining to the treatment of proximal humerus fractures. Choosing to focus on a different topic in the orthopedic literature may result in contrasting results. Thus, careful interpretation of our results on the frequency and influence of author COI in the orthopedic literature is warranted.
Conclusion:
In conclusion, our data shows a moderate rate of COIs in literature related to proximal humerus fracture treatments. COIs can result in design, analysis, and reporting bias, all of which can skew results. In contrast, our study found little reporting bias when there was a COI. It would be difficult to have physicians stop from getting incentives from industry and it has been suggested that industry payments help with the progression of research.25 As long as there is complete transparency with their COIs, authors of systematic reviews over proximal humerus fracture treatments should not be scrutinized for their bias affecting the results.
References
1. Horak J, Nilsson BE. Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res. 1975;(112):250-253.
2. Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006;37(8):691-697.
3. Lind T, Krøner K, Jensen J. The epidemiology of fractures of the proximal humerus. Arch Orthop Trauma Surg. 1989;108(5):285-287.
4. Fjalestad T, Hole MØ, Hovden IAH, Blücher J, Strømsøe K. Surgical treatment with an angular stable plate for complex displaced proximal humeral fractures in elderly patients: a randomized controlled trial. J Orthop Trauma. 2012;26(2):98-106.
5. Olerud P, Ahrengart L, Ponzer S, Saving J, Tidermark J. Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 2011;20(5):747-755.
6. Bell J-E, Leung BC, Spratt KF, et al. Trends and variation in incidence, surgical treatment, and repeat surgery of proximal humeral fractures in the elderly. J Bone Joint Surg Am. 2011;93(2):121.
7. Dall TM, Gallo PD, Chakrabarti R, West T, Semilla AP, Storm MV. An Aging Population And Growing Disease Burden Will Require ALarge And Specialized Health Care Workforce By 2025. Health Aff. 2013;32(11):2013-2020.
8. van Eck CF, Klein CM, Rahmi H, et al. Morbidity, mortality and cost of osteoporotic fractures—should proximal humerus fractures be taken as seriously as hip fractures? Annals of Joint. 2019;4:4-4. doi:10.21037/aoj.2019.01.01
9. Marx RG, Wilson SM, Swiontkowski MF. Updating the assignment of levels of evidence. J Bone Joint Surg Am. 2015;97(1):1-2.
10. Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. J Bone Joint Surg Am. 2003;85(1):1-3.
11. Scott J, Checketts JX, Cooper CM, Boose M, Wayant C, Vassar M. An Evaluation of Publication Bias in High-Impact Orthopaedic Literature. JB JS Open Access. 2019;4(2):e0055.
12. Lavis JN. How Can We Support the Use of Systematic Reviews in Policymaking? PLoS Med. 2009;6(11):e1000141.
13. ICMJE | Recommendations | Author Responsibilities—Disclosure of Financial and Non-Financial Relationships and Activities, and Conflicts of Interest. Accessed June 25, 2020. http://www.icmje.org/recommendations/browse/roles-and-responsibilities/author-responsibilities--conflicts-of-interest.html
14. Electronic Code of Federal Regulations- US Department of Health and Human Services’ Code of Federal Regulation 45 CFR 46.102(d). https://www.ecfr.gov/cgi-bin/retrieveECFR?gp=&SID=83cd09e1c0f5c6937cd9d7513160fc3f&pitd=20180719&n=pt45.1.46&r=PART&ty=HTML#se45.1.46_1102 in effect July 19, 2018
15. Ferrell M, Verble C, Anderson M, Weaver M, Hartwell M, Vassar M. Evidence of financial conflicts of interest in authors of proximal humerus repair systematic reviews and meta-analyses. Published online July 1, 2020. Accessed July 3, 2020. https://osf.io/4tzwy/
16. PRISMA. Accessed July 2, 2020. http://prisma-statement.org/
17. Murad MH, Wang Z. Guidelines for reporting meta-epidemiological methodology research. Evid Based Med. 2017;22(4):139-142.
18. Rulon Z, Jones CW, Ottwell RL. Evaluation of Spin in Systematic Reviews Related to the Management of Proximal Humerus Fractures. Published online May 29, 2020. Accessed July 3, 2020. https://osf.io/cvgtm/
19. Mandrioli D, Kearns CE, Bero LA. Relationship between Research Outcomes and Risk of Bias, Study Sponsorship, and Author Financial Conflicts of Interest in Reviews of the Effects of Artificially Sweetened Beverages on Weight Outcomes: A Systematic Review of Reviews. PLOS ONE. 2016;11(9):e0162198. doi:10.1371/journal.pone.0162198
20. Okike K, Kocher MS, Mehlman CT, Bhandari M. Conflict of Interest in Orthopaedic Research. The Journal of Bone & Joint Surgery. 2007;89(3):608-613. doi:10.2106/jbjs.f.00994
21. Narain AS, Hijji FY, Yom KH, Kudaravalli KT, Singh K. Cervical disc arthroplasty: do conflicts of interest influence the outcome of clinical studies? Spine J. 2017;17(7):1026-1032.
22. Kjaergard LL, Als-Nielsen B. Association between competing interests and authors’ conclusions: epidemiological study of randomised clinical trials published in the BMJ. BMJ. 2002;325(7358):249.
23. Bhandari M, Busse JW, Jackowski D, et al. Association between industry funding and statistically significant pro-industry findings in medical and surgical randomized trials. CMAJ. 2004;170(4):477-480.
24. Shnier A, Lexchin J, Romero M, Brown K. Reporting of financial conflicts of interest in clinical practice guidelines: a case study analysis of guidelines from the Canadian Medical Association Infobase. BMC Health Serv Res. 2016;16(a):383.
25. Boddapati V, Sachdev R, Fu MC, Camp CL, Marx RG, Dines JS. Increasing Industry Support Is Associated with Higher Research Productivity in Orthopaedic Surgery. J Bone Joint Surg Am. 2018;100(6):e36.
26. Lundh A, Lexchin J, Mintzes B, Schroll JB, Bero L. Industry sponsorship and research outcome. Cochrane Database Syst Rev. 2017;2:MR000033.
27. Khan SN, Mermer MJ, Myers E, Sandhu HS. The roles of funding source, clinical trial outcome, and quality of reporting in orthopedic surgery literature.Am J Orthop . 2008;37(12):E205-E212; discussion E212.
28. Hozack WJ, Ranawat C, Rothman RH. Corporate sponsorship and research. The Journal of Arthroplasty. 2003;18(8):953. doi:10.1016/j.arth.2003.10.009
29. Oostrom T. Funding of Clinical Trials and Reported Drug Efficacy.”. Published online 2020. https://pdfs.semanticscholar.org/ad9d/a7bf3d061116c6ae7515c651bb8c276b44df.pdf&hl=de&sa=X&d=2481165454991070009&scisig=AAGBfm0pU2GBj7xIJKqQECD8GYT0KYhv-Q&nossl=1&oi=scholaralrt&hist=76cO6AEAAAAJ:6061284773987871490:AAGBfm3WthEa5PhImJpHiGN_0yYVD3ZCNw
30. Friedberg M, Saffran B, Stinson TJ, Nelson W, Bennett CL. Evaluation of conflict of interest in economic analyses of new drugs used in oncology. JAMA. 1999;282(15):1453-1457.