Adrianna Elbon, OMS-III, Oklahoma State University for Health Sciences, College of Osteopathic Medicine Rural Medical Track
Krista Schumacher, PhD, Oklahoma State University Center for Health Sciences, Center for Rural Health
Corresponding author:
Krista Schumacher, OSU Center for Rural Health
Disclosures:This work received no external funding support. There are no conflicts of interest to disclose.
Abstract
Background
Although human papillomavirus (HPV) vaccination reduces infection and HPV-associated cancers, vaccination rates are low. The purpose of this study was to assess the relationship between vaccination status and health care provider recommendation and identify themes in provider messaging.
Methods
Using data from a survey of undergraduates, we used cross tabulation and chi-square analysis to examine the relationship between vaccination status and provider recommendation and coded qualitative responses to open-ended items about provider communication and influence.
Results
Vaccination status was significantly associated with provider recommendation. Just under half of vaccinated respondents with a recommendation received information beyond a simple recommendation, and 42% reported providers largely influenced their vaccination decision.
Conclusions
Reduced cancer risk was the most common topic in provider communication. Comments about provider influence suggest messages that convey a favorable opinion of HPV vaccination combined with education about risks associated with infection may positively sway vaccine decisions.
Keywords: Human papillomavirus (HPV), vaccine hesitancy, provider messaging
Introduction
Approximately 79 million individuals in the U.S. are infected with human papillomavirus (HPV), making it the most common sexually transmitted infection and one that most often occurs initially during the adolescent and young adult years.1 Although most HPV infections resolve on their own, several strains are linked to various types of cancer,2 with cases of HPV-associated cancers increasing by 50% from 1999 to 2017.3,4 In addition to vaginal, vulvar, penile, anal, and some oropharyngeal cancers, nearly all cases of cervical cancer are linked to HPV.5 HPV vaccination is particularly important in Oklahoma where cervical cancer incidence and mortality exceed national rates,6 yet HPV vaccination rates are lower than the U.S.7
Although HPV vaccination has been available in the U.S. since 2006,8 vaccination rates remain well below the U.S. Department of Health and Human Service’s Healthy People 2020 goal of 80% among ages 13-15 years.9 The quadrivalent Gardasil®-4, developed by Merck, was approved by the Food and Drug Administration (FDA) in 2006 to prevent cervical cancer.8 In 2014, the FDA approved the 9-valent Gardasil®-9, the only HPV vaccine currently available in the U.S., to prevent cervical, anal, and throat cancers. In 2020, the FDA extended approval to include oropharyngeal and other cancers of the head and neck.8
The Advisory Committee on Immunization Practices (ACIP) at the Centers for Disease Control and Prevention (CDC) recommends routine vaccination at ages 11-12 years, with a 2-dose schedule for ages 9-14, and “catch-up” vaccination for females and males through age 26, with a 3-dose schedule if initiated at age 15 or older.10,11 In 2020, the American Cancer Society released recommendations to vaccinate between ages 9-12 to promote more on-time vaccinations and encouraged clinicians to offer the vaccine series starting at ages 9-10.12 In addition, the American College of Obstetrics and Gynecology, American College of Family Physicians, and American Association of Pediatrics all recommend HPV vaccination.13–15
Prior to the COVID-19 pandemic, HPV vaccination rates had started to improve, and HPV infections caused by targeted subtypes fell by more than 60% among females aged 14-24 in the first 8 years following vaccine introduction.16 Data from the National Immunization Survey (NIS)-Teen show rates of U.S. adolescents aged 13-17 years who received at least one HPV vaccine dose increased steadily from 60.4% in 2016 to 75.1% in 2020; in Oklahoma, rates increased from 56.9% to 65.5%.7 The same trends occurred for percentage up-to-date (UTD), with national rates increasing from 43.4% in 2016 to 58.6% in 2020, and from 39.2% to 45.8% in Oklahoma.7
Although yearly increases occurred for both indicators at the state and national level, the gap between Oklahoma and the U.S. widened over time. Efforts to minimize this gap and maintain upward trajectories have been stalled due to the disruptions to preventive care caused by the COVID-19 pandemic. Because 2020 NIS-Teen data reflect vaccination coverage before the pandemic,17 Daniels et al16 modeled HPV vaccination coverage and showed declines of up to 77% from March to August 2020 compared to the same timeframe in 2019.16 Of particular concern is that vaccination already varied by geography, with rates for series initiation and UTD lower for youth living outside metropolitan statistical areas,17 for males compared to females,7 and for non-white racial/ethnic groups compared to whites.18 COVID-related declines in HPV vaccination are expected to contribute to substantial increases in cases of genital warts, cervical intraepithelial neoplasias (CIN), and cervical cancer.16 Thus, efforts to increase HPV vaccination rates are even more critical than before.
HPV vaccination rates are low among college students as well, with research pointing to a considerable gap in vaccine initiation and completion among this age group.19 Data from the National College Health Assessment (NCHA)-III for spring 2021 showed that just under half (49.4%) of respondents had completed the HPV vaccine series. An additional 21.8% had not received a single dose, 5% had started but not completed the series, and nearly one-fourth did not know their vaccination status.20 These statistics are similar for the prior three semesters.
Lack of provider recommendation has emerged as a key barrier to increasing vaccination rates,21,22 and research suggests provider recommendation for HPV vaccination is an important motivator for HPV vaccine initiation and series completion.23–26 However, not all providers recommend vaccination in the same way or for the same ages.27 A 2014 national survey of primary care physicians found that while nearly 75% believed recommending HPV vaccination was important, they recommended other routine vaccinations (e.g., Tdap) more often; conversations with parents about HPV vaccination were reportedly difficult, time consuming, and less likely to result in parental approval.28
Analyzing NIS-Teen data from 2012-2018, Sonawane et al29 found the rate of unvaccinated adolescents whose providers recommended the HPV vaccine grew from 27% in 2012 to nearly 50% in 2018; among these teens, parental reluctance to initiate the series increased from 50% to 64%. NIS-Teen data collected from January 2017 to 2019 showed Oklahoma was among states with the highest rates of vaccine hesitancy among parents of unvaccinated teens, with more than 65% refusing HPV vaccination.30 A detrimental relationship exists between parental vaccine hesitancy and provider communication about HPV vaccination. A review of the literature has shown providers who perceive parents to be resistant to vaccination are less likely to adhere to ACIP recommendations for HPV vaccination.31
All National Cancer Institute (NCI)-designated cancer centers have issued a consensus statement urging “health care providers to make clear and strong recommendations for HPV vaccination.”32 However, research on provider communication strategies and how they impact vaccination decisions, especially how they might overcome parental resistance, are limited.33–35 The purpose of this study was to assess the relationship between HPV vaccination status and provider recommendation and to understand whether particular themes in provider messaging were more prevalent than others.
Methods
We used a subset of data from a self-administered survey disseminated via email in fall 2020 to 5,000 undergraduates aged 18-24 enrolled at Oklahoma State University (OSU). The survey was approved by the OSU Institutional Review Board (IRB) and administered using the Qualtrics online survey tool. The survey consisted of quantitative items designed to measure HPV vaccine status, provider recommendation, perceived HPV risk, and HPV knowledge, as well as two open-ended items designed to explore provider communication and the extent to which communication influenced vaccine decision-making. Survey items selected for this study included quantitative items for HPV vaccine status (fully vaccinated, partially vaccinated (series started), not at all vaccinated, unsure), whether a health care provider ever recommended the HPV vaccine (yes, no), and the two qualitative items about provider communication.
This study aimed to 1) analyze the relationship between provider recommendation and vaccine status, 2) determine the percentage of vaccinated respondents with a provider recommendation who reported receiving communication beyond a simple recommendation, 3) identify salient themes in provider recommendations, and 4) assess the influence of provider communication on the vaccination decision.
We used a chi-square test to investigate whether vaccination status differed based on whether a provider recommendation was received and, if so, we used an odds ratio to examine the strength of the association. Respondents who reported being unsure about their status were excluded from the analysis. Assumptions for the chi-square test were checked and met. We used inductive open coding36 to manually code qualitative responses to the two open-ended items for respondents who indicated they were vaccinated and had received a provider recommendation. To identify themes in provider recommendations, we coded responses to the open-ended question “What information has a health care provider given you about HPV?” for content of provider communication. We then created a numerical variable to quantify communication content and used frequencies to identify salient themes. To assess the influence of provider communication, responses to the open-ended question “How did the health care provider influence your decision about HPV vaccination?” were coded for indications of strength of provider influence. Codes were combined into a numerical variable to quantify provider influence. We used SPSS v28 and Microsoft Excel 365 to analyze data and create new quantitative variables from open coding of qualitative data.
Results
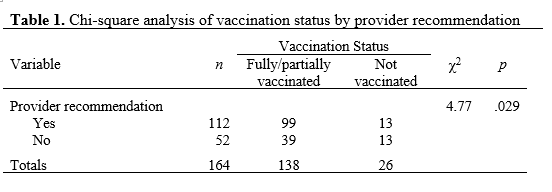
A total of 254 students responded to the survey, with 243 remaining after removing respondents with missing values on all items or all items except demographics. After excluding respondents who were unsure about their vaccination status (n=79), 164 respondents remained and consisted of mostly white (76.2%), females (70.1%), and from suburban hometowns (57.3%). The variable of HPV vaccination status was collapsed into a dichotomous variable that combined partially vaccinated (n=11) with fully vaccinated (n=127). Of remaining respondents, 84.1% were fully vaccinated or had started the series—of these 71% were female and 29% were male—and 68.3% reported having received a provider recommendation.
Table 1 shows the Pearson chi-square results and indicates that vaccination status was significantly different based on whether a provider recommendation was received (χ2 = 4.77, df = 1, N =164, p = .029). Vaccinated respondents were more likely than expected under the null hypothesis to have received a provider recommendation than unvaccinated respondents. An odds ratio was computed (OR = 2.54, 90% CI[1.24,5.20]) and indicated the odds of respondents being vaccinated if they had received a provider recommendation were 2.54 times as high as the odds for those who did not receive a recommendation.
Results of analyses of open-ended responses to qualitative items for vaccinated respondents with a provider recommendation (n=99) are discussed below. Quotes include participant (P) identification numbers to demonstrate scope of data coverage; male respondents are identified to show diversity of responses. About one-fourth (24%) of respondents did not answer the question about information received by a provider and 28% responded as unsure (e.g., “I don’t remember them telling ME anything, they spoke to my mom and got HER permission. It was all done prior to me turning 18” (P94, male)); nothing (e.g., “My health care provider gave little to no information and just gave me the shot” (P236)); recommended and nothing else (e.g., “That I should get it” (P30)); or the vaccine is available and nothing else (e.g., “I have prior knowledge of the vaccine and my health care provider simply asked if I found it necessary and wanted to receive the vaccine” (P60)).
Just under half (48%) of vaccinated respondents with a provider recommendation reported receiving provider communication beyond a simple recommendation. Coding revealed a few general categories: specific health consequences (e.g., cancer, genital warts), general comments about the vaccine (e.g., beneficial) or HPV (e.g., STI, common, dangerous), and use of written materials. Table 2 shows frequencies for specific provider messages reported by respondents and representative statements. The most common message related to cancer prevention, followed by use of written materials and statements that the vaccine is beneficial and reduces risk of HPV infection. Two respondents reported provider messages stating that HPV is a STI linked to certain cancers. To avoid duplication, these were coded with cancer messages.
For the open-ended question of how a health care provider influenced the vaccination decision, data were coded for whether responses indicated a large influence, some influence, no influence, or parents made the decision. Of 99 vaccinated respondents with a provider recommendation, 28% did not answer the question or indicated they were unsure or did not remember; 6% reported no influence; 2% said it was required for school entry or in their country; another 2% indicated being influenced at college age (e.g., “He told me that they recommend it for college students”(P75, male)); 5% said their provider somewhat influenced them (e.g., “I received a dose, but never went back for the others. I was swayed in the beginning but it didn't last” (P97); 14% noted either that providers spoke directly to their parents, or their parents influenced them (e.g., “He (provider) didn't influence my opinion either way. My mother influenced me to get it” (P161); and 42% reported a large degree of influence (e.g., “The health care provider influenced my decision because he is an expert regarding health” (P11, male); “A big influence, would never have known about the risks otherwise” (P151); “Without the doctor's input I would not have gotten (vaccinated)” (P175); “They seemed like they really wanted me to receive it” (P164, male)).

While the analysis for provider influence focused on vaccinated respondents with a provider recommendation, we examined the 13 responses that indicated a provider recommendation but were unvaccinated. Of these, four did not respond to question of influence; one expressed concern about adverse reactions (“The HPV vaccine is still a little too new for me to get. I have had many friends with adverse side effects...” (P63)); one expressed dissatisfaction with the provider conversation (“They… just made me feel guilty and wrong for not choosing to get it” (P78)); one indicated being unlikely to get vaccinated because “…I hate shots”(P170); three indicated receiving provider information about HPV and the need for vaccination but did not elaborate on why they refused (e.g., “I used to think HPV vaccination is only related to females, now I know that it is also important for a male to get HPV shots” (P109, male); and three indicated that their mom or parent refused the vaccine, which reflects the theme of parent resistance found in the literature: “Health care provider only asked if I would like to make an appointment to get it. Parents made final decisions” (P123, male); “(Health care provider) strongly recommended getting the vaccine. The only reason I didn’t get it is because my mom is against it” (P84); “(Health care provider) made me want one but my mom said no and at the time I couldn’t make that decision as a minor and I just haven’t taken the time since turning 18 to get it” (P10).
Discussion
This study identified salient themes in messages presented by providers when recommending HPV vaccination and demonstrated the extent to which favorable provider communication positively influenced vaccination decision-making. Our results are consistent with other studies that have found provider recommendation to be associated with greater vaccine initiation. Further, the findings from this study add to the scant research on provider messaging strategies. For this study sample, messages related to cancer prevention, benefits of vaccination, and use of written materials were most common. Although a small number of respondents indicated their parents objected to the vaccine, more indicated that their parents were the ones who made the decision to get them vaccinated. This points to the role that parental support plays in vaccine initiation and demonstrates the importance of educating and encouraging parents to have their children vaccinated.
This study has several strengths and limitations. Limitations include a small sample size comprised primarily of white female students from suburban communities. The study questionnaire used a self-report format, which may have introduced response bias. High vaccination rates among those reporting vaccination status could be an artifact of the survey attracting students who are familiar with HPV, while unvaccinated students may be less inclined to share their status, or they may feel the survey is irrelevant to them. There are inherent limitations in questions that ask for recall of an event that occurred many years ago. Several respondents stated that conversations either happened when they were early adolescents and could not be recalled or were geared toward their parents and not them. A few respondents who noted that providers positively influenced their decision to get vaccinated indicated they did not receive a provider recommendation, suggesting some provider recommendations were missing from the analysis.
Study strengths include the use of open-ended items that gave respondents the opportunity to share their experiences in their own words. This flexibility led to insights into the role of parents in the decision-making process (both positive and negative) as well as into potentially problematic provider messaging. For example, some respondents noted that providers stated HPV causes cancer in women or only focused on cervical cancer, which suggests providers did not discuss other cancers that can affect males. Of particular concern was communication recalled by a male respondent who said the provider indicated HPV would not “necessarily harm me but I could harm a future girlfriend.” This suggests either an incorrectly recalled conversation or a misunderstanding of HPV-related cancers by the provider.
Open-ended comments also revealed gaps in provider messaging, with respondents indicating that providers recommended the vaccine for protection against HPV without further explanation. It is important that individuals understand what HPV is and the cancers it can cause. Failing to educate patients represents a missed opportunity for these individual to encourage their friends to get vaccinated, especially among college-age populations. It also means that perceptions of a vaccine that has been available for years as “too new” are allowed to continue. The way providers communicate with patients is also important, as demonstrated by one respondent who said the provider made her feel “guilty and wrong” for refusing the vaccine. Shaming patients may reinforce vaccine hesitancy rather than reduce it and can amount to stigmatization, especially when a power differential exists such as that between a provider and patient, particularly a young patient.37
Further research is needed that examines patient-provider communication closer to the time it occurs as well as differences in the HPV vaccine decision-making process by different genders and racial/ethnic groups. Future studies among college-age populations should examine which specific provider messages serve as cues to action and how providers positively influence the vaccine decision.
Conclusion
HPV-related cancers are “a significant public health problem,”32 and the President's Cancer Panel considers increasing HPV vaccine uptake a public health priority in the U.S. and globally.38 In February 2021, the leaders of the American Academy of Family Physicians, American College of Physicians, American College of Obstetricians and Gynecologists, and the Immunization Action Coalition (IAC) issued a joint letter to colleagues urging “confident, clear, and consistent recommendation” for HPV vaccination.39 And in January 2021, the U.S. Department of Health and Human Services launched the HPV VAX NOW campaign to increase HPV vaccination rates among young adults aged 18-26.40
Numerous resources exist to help providers promote HPV vaccination, including the CDC’s on-demand webinar, You are the Key to HPV Cancer Prevention,41 and HPV information portal for providers, which includes infographics, clinical information (e.g., schedules, dosing, safety, efficacy), and the #HowIRecommend video series with tips for effective conversations with parents.42 The National Foundation for Infectious Diseases lists several resources for providers, including a 5-step infographic and policies and procedures (i.e., standing orders) issued by the IAC for administering HPV vaccines to children, teens, and adults.43 In 2018, Kognito Interactive released the app HPV Vaccine: Same Way, Same Day, which uses role-play simulation to help providers introduce the vaccine and alleviate parents’ concerns.44 Despite these resources, the literature suggests a large degree of inconsistency both in terms of when providers recommend vaccination and the messages used.27 Moreover, resources tend to focus on provider communication with parents, leaving a gap in resources for providers who see college-age students.
The findings from unvaccinated students who had received a provider recommendation in the past but whose parents objected demonstrate opportunities for colleges and universities to overcome the obstacle of parental resistance. College-age students are prime candidates for catch-up vaccination, and supportive recommendations from health care providers, particularly those at student health clinics, may positively influence vaccine uptake. Colleges and universities can use the Collegiate Vaccination Toolkit, developed by Project HPV Free,45 to conduct education and vaccination campaigns. Such efforts can serve to enhance awareness and increase vaccination rates among an age group nearing their last chance for vaccination.
REFERENCES
1. National Foundation for Infectious Diseases. HPV (Human Papillomavirus). January 2021. Accessed October 22, 2021. https://www.nfid.org/infectious-diseases/hpv/
2. Centers for Disease Control and Prevention. Genital HPV infection - fact sheet. January 19, 2021. Accessed September 20, 2021. https://www.cdc.gov/std/hpv/stdfact-hpv.htm
3. Van Dyne EA, Henley SJ, Saraiya M, Thomas CC, Markowitz LE, Benard VB. Trends in human papillomavirus–associated cancers — United States, 1999–2015. MMWR Morb Mortal Wkly Rep. 2018;67. doi:10.15585/mmwr.mm6733a2
4. Centers for Disease Control and Prevention. HPV-associated cancer statistics. September 16, 2020. Accessed October 21, 2021. https://www.cdc.gov/cancer/hpv/statistics/index.htm
5. Centers for Disease Control and Prevention. Cancers associated with human papillomavirus (HPV). September 14, 2020. Accessed October 21, 2021. https://www.cdc.gov/cancer/hpv/basic_info/cancers.htm
6. Gopalani SV, Janitz AE, Campbell JE. Trends in cervical cancer incidence and mortality in Oklahoma and the United States, 1999-2013. Cancer Epidemiol. 2018;56:140-145. doi:10.1016/j.canep.2018.08.008
7. Centers for Disease Control and Prevention. Vaccination coverage among adolescents (13-17 years). TeenVaxView. May 20, 2021. Accessed October 20, 2021. https://www.cdc.gov/vaccines/imz-managers/coverage/teenvaxview/data-reports/index.html
8. KFF (Kaiser Family Foundation). The HPV vaccine: access and use in the U.S. Women’s Health Policy. July 12, 2021. Accessed October 20, 2021. https://www.kff.org/womens-health-policy/fact-sheet/the-hpv-vaccine-access-and-use-in-the-u-s/
9. Immunization and Infectious Diseases | Healthy People 2020. HealthyPeople.gov. Accessed October 25, 2021. https://www.healthypeople.gov/2020/topics-objectives/topic/immunization-and-infectious-diseases/objectives
10. Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human papillomavirus vaccination for adults: updated recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2019;68. doi:10.15585/mmwr.mm6832a3
11. Meites E, Kempe A, Markowitz LE. Use of a 2-dose schedule for human papillomavirus vaccination — updated recommendations of the advisory committee on immunization practices. MMWR Morb Mortal Wkly Rep. 2016;65. doi:10.15585/mmwr.mm6549a5
12. Saslow D, Andrews KS, Manassaram-Baptiste D, Smith RA, Fontham ETH, Group the ACSGD. Human papillomavirus vaccination 2020 guideline update: American Cancer Society guideline adaptation. CA Cancer J Clin. 2020;70(4):274-280. doi:10.3322/caac.21616
13. Human papillomavirus vaccination: committee opinion number 809. The American College of Obstetricians and Gynecologists. July 23, 2020. Accessed August 5, 2021. https://www.acog.org/en/clinical/clinical-guidance/committee-opinion/articles/2020/08/human-papillomavirus-vaccination
14. Immunization schedules | Red Book Online | AAP Point-of-Care-Solutions. American Academy of Pediatrics. 2021. Accessed October 20, 2021. https://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=Immunization_Schedules
15. Human papillomavirus vaccine (HPV). American Academy of Family Physicians. 2021. Accessed October 20, 2021. https://www.aafp.org/family-physician/patient-care/prevention-wellness/immunizations-vaccines/disease-pop-immunization/human-papillomavirus-vaccine-hpv.html
16. Daniels V, Saxena K, Roberts C, et al. Impact of reduced human papillomavirus vaccination coverage rates due to COVID-19 in the United States: a model based analysis. Vaccine. 2021;39(20):2731-2735. doi:10.1016/j.vaccine.2021.04.003
17. Pingali C, Yankey D, Elam-Evans LD, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13-17 years - united states, 2020. MMWR Morb Mortal Wkly Rep. 2021;70(35):1183-1190. doi:10.15585/mmwr.mm7035a1
18. Cho D, Ramondetta L, Garcini L, Lu Q. HPVs vaccination among racial/ethnic minority college students: current status and future direction - clinicalkey. J Natl Med Assoc. 2020;112(6):639-649.
19. Rohde RL, Adjei Boakye E, Christopher KM, et al. Assessing university students’ sexual risk behaviors as predictors of human papillomavirus (HPV) vaccine uptake behavior. Vaccine. 2018;36(25):3629-3634. doi:10.1016/j.vaccine.2018.05.022
20. National College Health Assessment III, Spring 2021 Reference Group Data Report. American College Health Association; 2021. Accessed October 20, 2021. https://www.acha.org/documents/ncha/NCHA-III_SPRING-2021_REFERENCE_GROUP_DATA_REPORT.pdf
21. Bratic JS, Seyferth ER, Bocchini JA Jr. Update on barriers to human papillomavirus vaccination and effective strategies to promote vaccine acceptance.Curr Opin Pediatr. 2016;28(3):407-412. doi:10.1097/MOP.0000000000000353
22. Fokom Domgue J, Cunningham SA, Yu RK, Shete S. Reasons for not receiving the HPV vaccine among eligible adults: lack of knowledge and of provider recommendations contribute more than safety and insurance concerns. Cancer Med. 2020;9(14):5281-5290. doi:10.1002/cam4.3192
23. Stout ME, Christy SM, Winger JG, Vadaparampil ST, Mosher CE. Self-efficacy and hpv vaccine attitudes mediate the relationship between social norms and intentions to receive the HPV vaccine among college students. J Community Health. 2020;45(6):1187-1195. doi:10.1007/s10900-020-00837-5
24. Oh NL, Biddell CB, Rhodes BE, Brewer NT. Provider communication and HPV vaccine uptake: A meta-analysis and systematic review. Prev Med. 2021;148:106554. doi:10.1016/j.ypmed.2021.106554
25. Sriram S, Ranganathan R. Why human papilloma virus vaccination coverage is low among adolescents in the US? A study of barriers for vaccination uptake. J Family Med Prim Care. 2019;8(3):866-870. doi:10.4103/jfmpc.jfmpc_107_19
26. Ylitalo KR, Lee H, Mehta NK. Health care provider recommendation, human papillomavirus vaccination, and race/ethnicity in the US National Immunization Survey. Am J Public Health. 2013;103(1):164-169. doi:10.2105/AJPH.2011.300600
27. Lockhart S, Dempsey AF, Pyrzanowski J, O’Leary ST, Barnard JG. Provider and parent perspectives on enhanced communication tools for human papillomavirus vaccine–hesitant parents. Acad Pediatr. 2018;18(7):776-782. doi:10.1016/j.acap.2018.05.012
28. Gilkey MB, Moss JL, Coyne-Beasley T, Hall ME, Shah PD, Brewer NT. Physician communication about adolescent vaccination: how is human papillomavirus vaccine different? Preventive Medicine. 2015;77:181-185. doi:10.1016/j.ypmed.2015.05.024
29. Sonawane K, Zhu Y, Lin Y-Y, et al. HPV vaccine recommendations and parental intent. Pediatrics. 2021;147(3). doi:10.1542/peds.2020-026286
30. Sonawane K, Zhu Y, Montealegre JR, et al. Parental intent to initiate and complete the human papillomavirus vaccine series in the USA: a nationwide, cross-sectional survey. Lancet Public Health. 2020;5(9):e484-e492. doi:10.1016/S2468-2667(20)30139-0
31. Gilkey MB, McRee A-L. Provider communication about HPV vaccination: a systematic review. Hum Vaccin Immunother. 2016;12(6):1454-1468. doi:10.1080/21645515.2015.1129090
32. Rosenberg J. NCI-designated cancer centers endorse goal of eliminating hpv-related cancers. AJMC. June 13, 2018. Accessed October 25, 2021. https://www.ajmc.com/view/ncidesignated-cancer-centers-endorse-goal-of-eliminating-hpvrelated-cancers
33. Dempsey AF, O’Leary ST. Human papillomavirus vaccination: narrative review of studies on how providers’ vaccine communication affects attitudes and uptake. Acad Pediatr. 2018;18(2S):S23-S27. doi:10.1016/j.acap.2017.09.001
34. Fenton AT, Eun TJ, Clark JA, Perkins RB. Indicated or elective? The association of providers’ words with HPV vaccine receipt. Hum Vaccin Immunother. 2018;14(10):2503-2509. doi:10.1080/21645515.2018.1480237
35. Hopfer S, Clippard JR. College women’s HPV vaccine decision narratives. Qual Health Res. 2011;21(2):262-277. doi:10.1177/1049732310383868
36. Given LM, ed. Codes and coding. In: The SAGE Encyclopedia of Qualitative Research Methods. SAGE Publications, Inc.; 2008. doi:10.4135/9781412963909.n48
37. Silverman RD, Wiley LF. Shaming vaccine refusal. J Law Med Ethics. 2017;45(4):569-581. doi:10.1177/1073110517750597
38. HPV Vaccination for Cancer Prevention: Progress, Opportunities, and a Renewed Call to Action. A Report to the President of the United States from the Chair of the President’s Cancer Pane. President’s Cancer Panel; 2018:52. https://prescancerpanel.cancer.gov/report/hpvupdate/pdf/PresCancerPanel_HPVUpdate_Nov2018.pdf
39. LeRoy G, Fincher J, Phipps MG, Donovan D. Give a confident, clear, and consistent recommendation for HPV vaccine to increase uptake! Published online February 3, 2021. Accessed October 22, 2021. https://www.immunize.org/letter/recommend_hpv_vaccination.pdf
40. U.S. Department of Health and Human Services. HHS announces new HPV vaccination campaign for young adults and health care providers. January 6, 2021. Accessed October 22, 2021. https://www.hhs.gov/about/news/2021/01/06/hhs-announces-new-hpv-vaccination-campaign-young-adults-health-care-providers.html
41. Centers for Disease Control and Prevention. You are the key to HPV cancer prevention - 2018. March 29, 2021. Accessed October 22, 2021. https://www.cdc.gov/vaccines/ed/vaccine-communication/you-are-key-2018.html
42. Centers for Disease Control and Prevention. HPV: information for healthcare professionals. May 20, 2021. Accessed October 22, 2021. https://www.cdc.gov/hpv/hcp/index.html
43. National Foundation for Infectious Diseases. Best practices to increase hpv immunization rates. August 29, 2019. Accessed October 25, 2021. https://www.nfid.org/infectious-diseases/best-practices/
44. Kognito Interactive. HPV Vaccine: Same Way Same Day. 2018. Accessed October 23, 2021. https://apps.apple.com/us/app/hpv-vaccine-same-way-same-day/id1356847181
45. Project HPV Free. Collegiate vaccination toolkit. Accessed October 24, 2021. https://projecthpvfree.org/