Factors Related to Academic Success in First-Semester Osteopathic Medical Students
Emily Madrak, PhD, LAT, ATC., Assistant Professor, University of Virginia, Department of Kinesiology,Charlottesville, VA
Jennifer L Volberding, PhD, LAT, ATC., Department Chair, Professor, Athletic Training Program Director, Oklahoma State University Center for Health Sciences, School of Allied Health, Department of Athletic Training, Tulsa, OK
Jana Baker, DO, FACOI., Clinical Associate Professor., Oklahoma State University Center for Health Sciences., Tulsa, OK
Corresponding author: Emily Madrak
Assistant Professor
University of Virginia
Department of Kinesiology
Charlottesville, VA
Funding:N/A
Disclosures:N/A
Abstract
Background: Empirical evidence suggests that admission to medical school requires a strong undergraduate (UG) grade-point-average (GPA), UG science grade-point-average, and MCAT. However, factors such as self-efficacy and UG institution size have little investigation in their contributions to academic success in medical school. We hypothesized that self-efficacy and size of UG institution may lead to greater levels of academic success during the first semester of medical school.
Methods: An online survey was used to gather information on first-semester medical student self-efficacy and size of institution (observed through athletic division level). Students' first-semester GPA and class rank were retrieved and used as outcome variables defining academic success.
Results:UG GPA demonstrated significance with first semester GPA and class rank, respectfully: r=0.49, p<0.00; r= 0.55, p<0.00. UG science GPA demonstrated significance with first semester GPA and class rank, respectfully: r=0.53, p<0.00; r= -0.59, p<0.00.
Non-Division I schools demonstrated greater first semester GPA and class rank than Division I schools, respectfully: U(NndI=22, NdI=20)=110.5, z= -2.76, p<0.00; U(NndI=22, NdI=20)=102.00, z= -2.97, p<0.00.
Conclusions: Those with degrees from smaller schools may have greater success in higher education. Future research should do a deeper investigate of UG institution size in comparison to academic success.
Key Words: academic success, Doctor of Osteopathic Medicine, medical school admissions, self-efficacy
Introduction
In general, the three domains utilized for medical school selection include general academic achievement, general aptitude (for example, the MCAT), and non-academic pursuits.5 In addition, medical schools typically require an interview, to assess personality and readiness for the rigor of medical education. On average, for every 22 applications, one student is accepted and enrolled, highlighting the competitiveness.6 The idea behind having a plethora of criteria is to select candidates who will develop into a “better” physician by the time the student graduates.7
In this research, we define academic success by academic achievement, operationalized by GPA and class rank.8 General academic achievement is typically estimated utilizing undergraduate (UG) and/or graduate grade point average (GPA), which provides an objective measure and allows for direct comparison of applicants. A foundation in natural science and mathematics has traditionally been sought after for applying to medical school, which has shown to be a precursor for academic success.9,10 The MCAT is also considered during the admissions process, which gives an additional objective measure of comparison to assess readiness and potential success.11 Additional research demonstrates that MCAT scores are strong predictors of the United States Medical Licensing Examination (USMLE) step 1 and verbal reasoning scores (prior to 2015), presenting the most predictive value in clinical performance in clerkship and residency. Furthermore, those who had lower scores (in general and in verbal reasoning) exhibited more difficulty in medical school.12
Previous research suggests that candidates who are selected based upon previous academic achievement and desirable personality traits will achieve more academic success in the first year.9,10,11 Because of this combination of academic ability and desired personality traits, we are interested in determining what combination will best help students achieve academic success, especially within their first semester.5 We hypothesize that age, gender, race/ethnicity, language background, size of hometown, number of applications, science-based UG degree, certificate or participation in the Bridge Program, public or private UG institution, choice of accepted medical schools, highest level of education attained by the students’ parents, and size of UG institution (represented by athletic division) may all have an impact on academic success within the first semester.
In addition to the personal and academic factors, we hypothesize that self-efficacy will play a role to academic success. Self-efficacy is derived from Bandura’s13 self-efficacy theory and is defined as the ability to believe in one’s actions and the execution in them to produce given attainments.13 It is related to an individual’s drive to succeed, dealing with adversity, and coping with challenges.14 Self-efficacy theory research in other disciplines demonstrates links between the effects of greater self-efficacy and greater academic achievement.14 Currently, there is a lack evidence linking self-efficacy and academic success with DO students.
Methods
Setting and Participants
This research was executed at a College of Osteopathic Medicine (COM). During the fall semester, 42 first-year medical students were recruited via email and during orientation. Participation was voluntary; information was provided containing the aims of the study within the first portion of the survey. An institutional review board (IRB) approved this research. Informed consent for each participant was gathered electronically.
Instrumentation
An observational study was completed with an online survey. The first portion of the survey contained questions of age, gender, race/ethnicity, language background, size of hometown, number of applications, science-based UG degree, certificate or participation in the Bridge Program (a year-long program that assists in entry into the COM for disadvantaged, medically underrepresented backgrounds, or those pursing medicine as a second career prior to entering the COM), public or private UG institution, choice of accepted medical schools, highest level of education attained by the students’ parents, UG athletic division (Division I or Non-Division I, used to gauge size of the institution).15 It is noteworthy to include that in order to best maintain confidentiality, asking the size of athletic division at the institution was the best way to approximate school size, as Division I schools are usually larger than other divisions. In addition, UG GPA, UG science GPA, highest MCAT score, MCAT score, and class ranking were retrieved from academic affairs databases for data analysis. Once the semester was complete, the students’ first semester GPA and class rank were retrieved after a de-identification processes was executed. Self-Efficacy was measured using the Sherer et al. General Self-Efficacy scale.16
The Sherer et al16 General Self-Efficacy Scale (SGSES) was used in subscale form: General Self-Efficacy (GSE) and Social Self-Efficacy (SSE), which have Cronbach’s alpha reliability measures equaling of α = 0.86 and α = 0.71, respectively.16 The survey utilized a Likert-scale with 14 points ranging from strongly disagree to strongly agree. The scale has a maximum score of 322; when divided, GSE is maxed out at 238 and SSE is maxed out at 84.16 It includes 23 questions; 17 general and 6 social.16 Those who score higher on the general scale are normally competent and show little difficultly in few areas.16 Those with higher scores on the social scale may indicate better ability in keeping a job rather than academic success.16
Data and Analysis
Survey data was entered into IBM SPSS 24.0 for analysis. Both self-efficacy sub-scales were summed and scored for each participant. A Pearson correlation analysis was used to analyze the comparison of continuous variables: UG GPA, UG science GPA, MCAT Highest score, 2015 MCAT, GSE, SSE with the outcome variables: first-semester medical school GPA and first-semester medical school class rank. Categorical variables, such as gender, race/ethnicity, language background, parent/guardian level of education, size of hometown, size of UG institution (athletic division), certificate or bridge program, public or private UG institution, science-based UG degree, choice of medical school, and total number of applications submitted were compared against first semester medical school GPA and first semester medical school class rank used Mann Whitney Tests. Significance level for all statistical analyses was measured at α=0.05.
Results
The Pearson correlation revealed significant correlations in three different areas. Table 1 displays the descriptive statistics and Pearson Correlations. Although we initially hypothesized that self-efficacy would have a strong impact on academic success, it did not prove to be significant with first-semester class rank or GPA.
Table 1
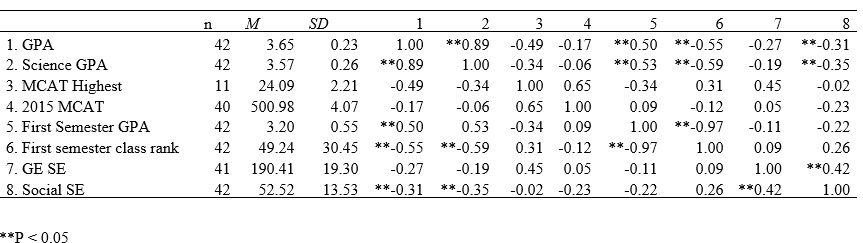
Descriptive Statistics and Pearson Correlation
Note: **p<0.05
Undergraduate GPA and first semester GPA, respectfully: r=0.49, p<0.00. UG science and first-semester GPA: r=0.53, p<0.00. A moderate positive-sloped correlation is demonstrated for each of these, suggesting that as the level of the variable increases, the first semester GPA increases. Undergraduate GPA and first-semester class rank: r= -0.55, p<0.00. Undergraduate science GPA and first-semester class rank: r= -0.59, p< 0.00. Moderate negative-slope correlations are demonstrated for each of the variables for class rank, indicating that as the variation of GPA decreases, the class rank increases. Due to ranks being observed in reverse in academia a class rank of “1” is greater than “120.”
Size of UG institution (athletic division) and both first semester GPA and class rank demonstrated significance with Mann Whitney tests. The Mann Whitney test indicated that first semester GPA was greater for non-Division I undergraduate (Mdn=3.50) than Division I undergraduate (Mdn=2.92), U(NndI=22, NdI=20)=110.5, z= -2.76, p<0.00. The Mann Whitney test for first semester class rank was greater for non-Division I undergraduate (Mdn=30.5) than Division I undergraduate (Mdn=65.6), U(NndI=22, NdI=20)=102.00, z= -2.97, p<0.00.
Discussion
This study aimed to explore what combination of academic ability and desired personality traits will best help DO students achieve academic success, especially within their first semester. Our initial hypothesize included a variety of personal factors (age, gender, race/ethnicity, language background, size of hometown, number of applications, science-based UG degree, certificate or participation in the Bridge Program, public or private UG institution, choice of accepted medical schools, highest level of education attained by the students’ parents, and size of UG institution (represented by athletic division)) may all have an impact on academic success within the first semester. Through demographic questions and the Self-Efficacy Scale16, we found significant outcomes between a small group of factors and how they impacted a first-semester GPA and class rank.
Undergraduate GPA and Undergraduate Science GPA
Undergraduate GPA and undergraduate science GPA show affirmative impacts on first-semester COM GPA and class rank. The results reflect the outcome of previous studies relating to undergraduate GPA and Osteopathic medical student academic success.17,18 Furthermore, the results are consistent with previous research, stating that mental abilities (specifically, academic ability), can significantly predict future performances.5 In addition, previous research indicates those who have a stronger science background may in-turn have stronger reasoning skills, specifically related to clinical reasoning.10,19 This is notable, because to have strong clinical reasoning, the student needs to accurately analyze what the problem is, and apply a basic science concept to it that has deep conceptual knowledge tied to it, rather than just observing at face value, which can lead to misinterpretation of the possible procedure needed.10 A strong theoretical ground is needed to achieve this, including better explanations, clarifications, and promotion of the clinical application of basic science concepts.10 This is noteworthy for further exploration of how academic success can relate to clinical skills.
Size of Undergraduate Institution (Athletic Division)
Because of the significant outcome with Non-Division I schools and academic performance in the first year of DO school, a smaller university with smaller class sizes may relate to enhanced academic success. We used size of the athletic division at the participant’s undergraduate institution to gauge how large the school was. Division I schools are usually larger (in terms of student population) than Non-Division I, indicating a large student-to-faculty ratio. Size of class is a well-researched subject, which has demonstrated better performance on essay and mid-semester examinations in smaller classes, but scores on quizzes and final examinations had better performance in large classes.20 However, new research has since emerged indicating those in tougher disciplines, such as biological, physical, and chemical sciences, and engineering have greater scores with smaller class sizes of 10, rather than 50 or greater.21 Larger class sizes are often less personal, associated with traditional teaching methods such as lecturing, and require less involvement with peers and faculty, which can diminish the success of the student.21 Smaller classes often have more engagement and incorporate more progressive teaching methods, such as “active” learning, where the students are actively engaged in the learning process and tend to be more effective on student success as a result.21 Future research should do a deeper investigation of UG institution size.
Limitations
Though we unveiled many pieces of important information in our research, it was not without limitation. First, all data was drawn from one institution which may alter the generalizability of the data. Second, our sample size was small. A larger sample may have demonstrated significance with self-efficacy. Finally, other variables that were evaluated did not have the statistical significance we anticipated. For example, the MCAT was found to have correlations with academic success in various other Osteopathic medical student studies, but ours lacked reportable significant findings.17, 18 Additionally, we did not ask participants for their personal characteristics such as gender, age, ethnicity, etc. This is noteworthy to consider for the future.
Conclusion
In summary, our research indicates that previous academic success during undergraduate school and smaller universities will yield greater academic success for DO students within their first year. This is noteworthy not only for medical school admissions committees during their selection process, but for prospective students. Our research suggests the importance of other factors beyond academics, such as the size of the university and the variability between applications to achieve the greatest academic success in DO school. Future research should investigate clinical experiences and residency, using the interview process as a variable, and the Comprehensive Osteopathic Medical Licensing Examination (COMLEX) as an outcome variable.
Acknowledgements
A special thank you to Stephanie Link, PhD, Associate Professor, Director of Graduate Studies, Director of International Composition Program, Department of English, Oklahoma State University, for her contributions to this research.
Declarations of Interest
Ethics approval and consent to participate: This study was approved by an institutional review board and meets all criteria for working with human subjects.
Competing interests: No potential competing interest was reported by the authors.
Funding: Not applicable.
Authors' contributions: JV and JB made substantial contributions to the conception and design of this research. JV and EM made substantial contributions to the analysis and interpretation of data. EM drafted the work while JV and JB substantively revised it. All authors have approved the submitted version of this manuscript. All authors agreed to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
References
1. Guerrasio J, Garrity MJ, Aagaard, EM. Learner deficits and academic outcomes of medical students, residents, fellows, and attending physicians referred to a remediation program, 2006–2012. Acad Med. 2014; 89(2): 352-358 doi: 10.1097/ACM.0000000000000122
2. AAMC Graduation rates and attrition rates of U.S. medical students. Association of American Medical Colleges. https://www.aamc.org/download/492842/data/graduationratesandattritionratesofu.s.medicalstudents.pdf. Updated 2018. Accessed June 15, 2019.
3. AACOM Osteopathic medical school attrition summary. American Association of Colleges of Osteopathic Medicine. https://www.aacom.org/docs/default-source/data-and-trends/2009-10-to-2018-19-comattritsumm.pdf?sfvrsn=a4416197_12. Updated 2019. Accessed August 29, 2019.
4. AAMC Graduation rates and attrition factors of U.S. medical school students. Association of American Medical Colleges. https://www.aamc.org/download/379220/data/may2014aib-graduationratesandattritionfactorsforusmedschools.pdf. Updated 2014. Accessed June 15, 2019.
5. Hecker K, & Norman G. Have admissions committees considered all the evidence? Adv Health Sci Educ Theory Pract. 2017; 22: 573-576. https://doi.org/10.1007/s10459-016-9750-1
6. AACOM Enrollment and graduates by osteopathic medical college. American Association of Colleges of Osteopathic Medicine. https://www.aacom.org/docs/default-source/data-and-trends/applications-enrollment-and-graduates-by-osteopathic-medical-college-2014-2019.pdf?sfvrsn=a6d83497_7. Updated 2019. Accessed August 29, 2019.
7. Stegers-Jager KM. Lessons learned from 15 years of non-grades-based selection for medical school. Med Educ. 2017; 52(1): 86-95. https://doi.org/10.1111/medu.13462
8. York TT. Defining and measuring academic success. Practical Assessment, Research & Evaluation. Res High Educ. 2015; 20: 1-19. https://doi.org/10.7275/hz5x-tx03
9. Hirshfeild LE, Yudkowsky R, & Soo Park Y. Pre-medical majors in humanities and social sciences: Impact on communication skills and specialty choice. Med Educ. 2019; 53: 408-416. https://doi.org/10.1111/medu.13774
10. Castillo J, Soo Park Y, Harris I, Cheung JJH, Sood L, Clark MD, Kulasegaram K, Brydges R, Norman G, & Woods N. A critical review of transfer of basic science knowledge in health professions education. Med Educ. 2018; 52: 592-604. https://doi.org/10.1111/medu.13519
11. Skylar DP. Preparation for medical school: Reflections on the MCAT exam, premedical education, and the medical school application process. Acad Med. 2013; 88(5): 553-554. doi: 10.1097/ACM.0b013e31828b7c8f
12. Lisenmeyer M. & Ridpath L. Nelson-Denny reading test scores as a predictor of student success in osteopathic medical education. J Am Osteopath Assoc. 2019; 119(3): 189-197. https://doi.org/10.7556/jaoa.2019.030
13. Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977; 84: 191-215. https://doi.org/10.1037/0033-295X.84.2.191
14. Chemers MM, Hu L, & Garcia BF. Academic self-efficacy and first-year college student performance and adjustment. J Educ Psychol. 2001; 93: 55-64. https://pdfs.semanticscholar.org/9ddc/a7c27f179aae376ea8016b984421aea31d6a.pdf
15. Bridge Program. Oklahoma State University Center for Health Sciences. https://health.okstate.edu/com/admissions/bridge-program.html. Updated 2019. Accessed August 29, 2019.
16. Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, & Rogers RW. The self-efficacy scale: Construction and Validation. Psychol Rep. 1982; 51: 663-671. 10.2466/pr0.1982.51.2.663
17. Agahi F, Speicher MR, Cisek G. Association between undergraduate performance predictors and academic and clinical performance of osteopathic medical students. J Am Osteopath Assoc. 2018; 118: 106-114. https://doi.org/10.7556/jaoa.2018.025
18. Dixon M. Prediction of osteopathic medical school performance on the basis of MCAT score, GPA, sex, undergraduate major, and undergraduate institution. J Am Osteopath Assoc. 2011; 112: 175-181. Doi: 10.1007/s10459-016-9681-x
19. Lambe P, Bristow D. Predicting medical student performance from attributes at entry: a latent class analysis. Med Educ. 2011; 45(3): 308-316. https://doi.org/10.1111/j.1365-2923.2010.03897.x
20. Edmonson JB, Muldek FJ. Size of class as a factor in university instruction. J Educ Res. 1924; 9(1): 1-12, doi: 10.1080/00220671.1924.11431606
21. Johnson IY. Class size and student performance at a public research university: A cross-classified model. Res High Educ. 2010; 51: 701-723. https://www.jstor.org/stable/40927276
22. Heinisch BJ. Rural students’ sense of belonging at a large public university [dissertation]. Lincon, NE: University of Nebraska; 2018.
23. Zajacova A, Lynch SM, & Espenshade TJ. Self-efficacy, stress, and academic success in college. Res High Educ. 2005; 46: 677-706. https://doi.org/10.1007/s11162-004-4139-z