Emotional Intelligence Levels in Professional Athletic Training Students
Jennifer L Volberding PhD, ATC., Oklahoma State University Center for Health Sciences
W David Carr PhD, ATC., Missouri State University
Haddon M McIntosh BS., Oklahoma State University Center for Health Sciences
Luke C Weaver BS., Oklahoma State University Center for Health Sciences
Rileigh Ricken BS., Oklahoma State University Center for Health Sciences
No funding sources and no conflicts of interest to disclose
Background: Recent evidence suggests that a major factor in patient satisfaction and practitioner happiness in health care may be emotional intelligence (EI), or the ability to recognize and modulate the emotions of oneself and others. Literature has demonstrated that EI has decreased in health care providers.
Objective: This study sought to find differences in EI levels of bachelors and master’s level athletic training (AT) students.
Design: Cross Sectional Analysis
Setting: Bachelors and master’s level professional programs.
Participants: Snowball sampling through program directors yielded 44 bachelor’s and 35 master’s students.
Method(s): Self-reported opinions of EI were collected via the Schutte Emotional Intelligence Scale (EIS). Two one-way ANOVAs were conducted to determine if there were mean differences in EI between degree level and gender. Pearson correlations coefficients were conducted to examine the association between age and EI.
Results: There were no significant differences in bachelor’s and master’s student’s EIS scores, however, a gender difference was noted, with males scoring higher. There was a significant correlation between age and EIS score.
Conclusions: This project demonstrates EI differences in men and women that are not supported by past research and should be further explored. EI education should be included in AT curricula to slow the downward trend in EI and improve the health care experience for practitioners and patients.
Key Words: Patient-based care, professional preparation, patient interactions
Introduction:
The need for excellent bedside manner is not a novel idea in health care, however, recent studies indicate that beyond presenting with a positive and friendly attitude, practitioners should be skilled at recognizing emotions in patients and have the ability to adapt to them.1, 2 Emotions play a pivotal role in the patient-provider interaction. Health care providers skilled at interpreting emotions has shown higher rates of patient satisfaction and compliance to care plans designed for patients.1
Emotional intelligence (EI) includes the ability to recognize or manage, one’s emotions and the emotions of others.3,4 EI is characterized by five components: self-awareness, self-regulation, motivation, empathy, and social skills.5 Self-awareness can be defined as knowing one’s strengths and limitations. Self-awareness is directly linked to making healthy decisions when presented with difficult emotional situations. The second component, self-regulation can be defined as the act of exercising influence of your own behavior when experiencing emotion.6 The third component, motivation, is described as having the persistence to move toward your goals, feeling hope, and optimism while working toward an objective.7 Empathy has been described as “the brake on human cruelty,” if you can understand how your actions are hurting others, empathy may compels you to stop that action.5 The fifth component of EI is social skills, which includes any personal trait necessary to successfully communicate and interact with others.
Emotional intelligence has been shown to be a more accurate predictor of success than intelligence measured by IQ.7 Success in relationships, schools, careers, and physical health are all positively affected by increased EI. EI training allows for student growth in empathy, motivation, and social interaction. EI is important for athletic trainers (ATs)8; however, much of the literature is focused on physicians and nurses. ATs work with clients in emotional distress and would benefit from high levels of applied emotional intelligence. Practitioners who exhibit low emotional intelligence are more prone to burnout with decreased job and patient satisfaction.9 Inadequate relationships between the practitioner and patient can be a detriment to patient recovery.2 A physician’s EI has been shown to have positive effects on patient trust, patient-physician relationship, and patient satisfaction.10 The importance of EI in health care is understood within the field, however, EI has been shown to be significantly decreased in recent generations, such as millennials.1 It is possible the variables leading to diminished EI in millennials will lead to further regression of EI amongst Gen Z and subsequent generations.11
Previous research has demonstrated contradictory findings regarding sex differences related to EI. The author of the Emotional Intelligence Scale (EIS), Schutte, found female students demonstrated higher emotional intelligence compared to males 12, whereas Petrides & Furnham found no difference in EI between males and females.13
Facets of EI can be improved via EI education with: “(1) professional discourse about skills techniques, research, and special cases; (2) authentic experience or actual hands-on experience; and (3) skill development or time for skill instruction, practice, role-playing,
and simulations”17 during (AT)education. However, there are barriers to using teachable moments during clinical education alone. While educating students in the clinical settings, providing care for athletes must take priority at times. The ability to increase individual EI during undergraduate and graduate studies can be accomplished without interference to classroom performance.14, - 16
A pilot study was performed on EI of undergraduate and first-year master’s level AT students at two Midwest universities. Results showed low EI scores in both groups with no significant differences.18 The purpose of this study was to determine if there is a difference in the EI between an undergraduate and professional master’s level Athletic Training student.
On average, graduate students are older and more academically and professionally experienced than many undergraduate students. Whether this correlates to differences in EI between these two categories of AT students remains to be parsed out in the literature. A small pilot study at two Midwestern Universities with the current instrument found no significant differences in EI between graduate and undergraduate AT students.18 The purpose of this study was to conduct a study of students from a variety of universities to determine if EI levels in undergraduate versus graduate master’s level AT students differs.
Methods:
Participants
Convenience sampling was utilized to recruit Program Directors from accredited AT Programs. Program Directors of 29 undergraduate AT and 29 Entry-Level Master’s programs were made aware of the study via email and phone calls from the Principal Investigator, and then emailed the survey URL link. All study invitees were emailed the survey URL via Program Director. Students surveyed were enrolled in the professional phase of the AT programs at various universities in the United States. Due to the snowball sampling strategy utilized, a response rate was unable to be calculated. The Human Subjects Review Board approved the study and informed consent was obtained via electronic consent as part of the survey data collection.
Instrumentation
The Schutte Emotional Intelligence Scale (EIS) was selected for use during this study due to its reliability and validity shown in past athletic training research.12, 18, 19 The EIS is comprised of 33 statements where participants are asked to rate items on a 5-point Likert scale ranging from 1(strongly disagree) to 5 (strongly agree). Responses to each item were summed to form a composite score which ranged from 33 to 165. Schutte’s cross-check for internal consistency measured a Cronbach’s alpha of 0.87, which was determined appropriate for this study by the survey author.12 Cronbach’s alpha for the current study was also determined to be appropriate with a calculated value of 0.64.
Data Analysis
Analyses were performed using SPSS 20 (SPSS Inc., Chicago, IL). Two one-way ANOVAs were performed for undergraduate versus entry-level master’s students EI scores and male versus female EI scores, an alpha level of 0.05 used to determine significant results. A Pearson two-tailed correlation test was also performed to measure the correlation between age and composite EI score following the ANOVA test.
Results:
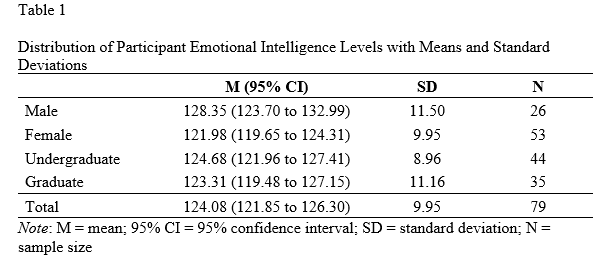
Seventy-nine students (male = 26, female = 53, undergraduate = 44, master’s = 35, average age = 22.42 + 4.41, undergraduate average age = 21.20 + 1.65, master’s average age 23.94 + 6.07) completed the survey. Table 1 shows descriptive statistics for the participant population as well as EI composite score means and standard deviations. The composite score ANOVA for undergraduate versus master’s students was determined to not be statistically significant (F (1, 77) = .365, p = 0.55, η2=0.005). The one-way ANOVA to compare male versus female composite EI scores did demonstrate significance (F (1, 77) = 7.76, p = .01, η2= 0.091). The two-tailed Pearson correlation coefficient was significant at the 0.01 level for a moderate, negative correlation between age and composite EI score (r = -0.32, p <.01).
Discussion:
The importance of EI in AT students lies in their future in the health-care industry. Patient care encompasses proper treatment as well as any patient interaction that pertains to their healing. The findings of this study found the low EI cumulative scores of both groups are in line with findings on millennial students. Athletic trainers with low EI
scores, when compared to other research, may lack the empathy or social skills required to put patients at ease during a difficult time. This can lead to previously stated issues with the patient perception of care provided as well as decreases in job satisfaction for the practitioner.9, 10 This is most likely due to a multitude of factors and has led many researchers to recommend the addition of emotional intelligence education to higher education curriculum.20
This study found there are no differences in EI cumulative scores between AT students at the professional undergraduate and master’s levels. However, there is a moderate correlation between EI scores and age, which would agree with data from the past that suggest EI scores improve with age.11 The results did show a significant difference between the EI scores of male and female students, with males scoring significantly higher, which conflicts with past findings.12
The findings from this research also suggest that AT curriculum could benefit from considering the addition of emotional intelligence instruction. Previous research demonstrated AT students with a higher EQ (mean of 127.16) compared to the current findings (mean of 124.08). Due to the relatively low EI scores, emotional intelligence training should be considered when planning curricula and class structures, and not only expected during clinical education opportunities. This training could be helpful for students and their future patients. EI intervention studies have shown that lasting improvements have been made with as little as 10 hours of EI education.14
Acknowledging the demanding didactic and clinical education hours typical in AT programs, EI training may take some reorganization, but would most likely be a beneficial addition.
Limitations and Future Research
This study used a small sample size of just 79 students and a re-evaluation of these results will be necessary in the future once all AT programs are master’s level degrees. Given the limitations, the current study expanded upon previous research on EI in AT students, more research on the topic is necessary to find if the inclusion of EI education would enhance or harm the current AT program curriculum. Research on gender differences in EI scores is warranted with a larger population to determine if the findings of this study hold true within a larger population. Future projects could compare gender differences in EI to those in other disciplines.
Conclusions
Higher EI scores in practitioners have shown to be beneficial for the provider and patient. Using methods to increase EI in AT students could lead to better handling of emotional situations, more effective communication with patients, and higher patient satisfaction.8-10 Improvements in EI of AT students and practitioners would inevitably create a positive change in the future of healthcare.
References
1. Dubé L, Bélanger MC, Trudeau E. The role of emotions in health care satisfaction. Marketing Health Services. 1996;16(2):45-51.
2. McQueen AC. Emotional intelligence in nursing work. J Adv Nurs. 2004;47(1):101-108.
3. Solovey P, Mayer JD. Emotional intelligence. Imagin Cogn Pers. 1990;9(3):185-211.
4. Thorndike EL. Intelligence and its uses. Harper's Magazine. 1920;140:227-235.
5. Goleman D. Emotional intelligence. New York, NY: Bantam Books; 1995.
6. Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Process. 1991;50(2):248-287.
7. Pool CR. Conference Report: Up With Emotional Health. Educ Leadersh. 1997;54(8):12-14.
8. Eberman LE, Kahanov L. Emotional intelligence: A requisite for good clinical practice. Athl Educ Train J. 2011;6(3):127-128.
9. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45(8):835-842.
10. Weng HC. Does the physician's emotional intelligence matter?: Impacts of the physician's emotional intelligence on the trust, patient-physician relationship, and satisfaction. Health Care Manage Rev. 2008;33(4):280-288.
11. Konrath SH, O'Brien EH, Hsing C. Changes in dispositional empathy in American college students over time: a meta-analysis. Pers Soc psychol Rev. 2011;15(2):180-198.
12. Schutte NS, Malouff JM, Hall LE, et al. Development and validation of a measure of emotional intelligence. Pers Individ Dif. 1998;25(2):167-177.
13. Petrides KV, Furnham A. Gender differences in measured and self-estimated trait emotional intelligence. Sex Roles. 2000;42(5-6):449-461.
14. Nelis D, Quoidbach J, Mikolajczak M, Hansenne M. Increasing emotional intelligence: (How) is it possible?. . Pers Individ Dif. 2009;47(1):36-41.
15. Pool LD, Qualter P. Improving emotional intelligence and emotional self-efficacy through a teaching intervention for university students. Learn Individ Differ. 2012;22(3):306-312
16. Boyatzis RE, Stubbs EC, Taylor SN. Learning cognitive and emotional intelligence competencies through graduate management education. Academy of Managt Learn & Educ. 2002;1(2):150-162.
17. Rich VJ. Clinical instructors’ and athletic training students’ perceptions of teachable moments in an athletic training clinical education setting. J Athl Train. 2009;44(3):294-303.
18. Hildebrand R, Volberding J, Carr WD. Examining Emotional Intelligence Differences in Athletic Training Undergraduates Students and First-Year Graduate Assistants. J Oklahoma Assoc for Health, Physl Educ, Recreation, and Dance. 2012;49(1):47-56.
19. Volberding JL, Baghurst T, Brown TC. Emotional intelligence levels of undergraduate kinesiology students: Brief report. N Am J Psychol. 2015;17(1):37.
20. McIntosh, H., Weaver, L., Ricken, R., Madrak, E., Volberding, J., Harrison, A., Bray, N., Farrar, N., Murray, K., O’Brien, M., Wymore, R., Davidson, B., Drinnon, S. “Improving Interprofessional Practice & Cultural Competence with Interprofessional Education.” Poster presentation, September 10, 2022, OSU-COM at the Cherokee Nation, Tahlequah, Oklahoma.