Discussion
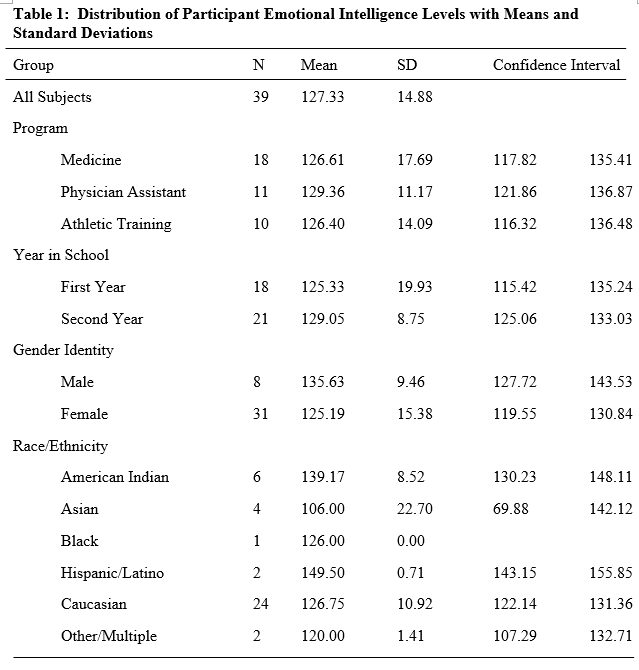
Emotional intelligence is an invaluable component to the competency of healthcare providers. Therefore, it is important for students in healthcare educational programs to learn, develop, and demonstrate the qualities of EI. In doing so, students will be equipped for effective, mutually beneficial interaction with future patients. Seeking to evaluate EI differences in students across healthcare educational programs, this study determined EI levels of MS, AT, and PA students. Additional considerations were given to differences in year in school, gender, and race/ethnicity. Overall mean EI scores in the study’s population were consistent with previous research done on comparable populations with similar demographics. The overall mean EI score for the student populations were slightly higher than but still consistent with previous research using similar EI measurements.16,17 However, males in this study demonstrated higher overall EI scores than females, inconsistent with the body of EI research.3,18,19 One plausible explanation for this difference was the average age of each group, where male respondents were much older than females. Increased age is associated with higher EI 5. Additionally, the conscious competence model published by Keeley20 provides a potential explanation. According to this framework, there is a hierarchy of competence amongst medical trainees. Unconscious incompetence, the beginning of this hierarchy, is a state where trainees lack the skills needed to excel. They are also unconsciously unaware of their deficiencies, potentially ascribing to a false sense of ability due to their ignorance. In this study, unconscious incompetence could account for a false elevation of perceived EI amongst the male population. On the other hand, women in the study may have been more conscious of their EI incompetence, scoring lower on EI measures, and accounting for the male/female disparity. While considering these explanations, an obvious truth remains; gender is an important piece of personhood. These findings suggest it has a great influence on functional EI.
The findings demonstrated no statistically significant differences in cumulative EI scores between MS, PA, and AT students. Additionally, they suggested no statistically significant difference in EI between first- and second-year students in their respective training programs. This study is consistent with past research that suggests no significant differences in EI across health-related disciplines. 17 However, previous research found that EI levels were higher for individuals in undergraduate programs as compared to first year professionals, suggesting a decrease in EI from the beginning of training through the first year in the workplace.16 This study expands upon that previous finding, suggesting the decrease is not accounted for by the transition from first-year to second-year student status, as no significant differences in EI were found between first- and second-year students. Rather, this EI decrease may potentially occur later in training, after entering the workforce, or in a continual manner as curricula advances across training programs. This finding is helpful to the overall EI discussion, but it still does not explain the origin of the observed drop off. The timing of and reasoning behind this data point may prove difficult to determine.
This study also found some noteworthy differences in EI in regard to race and ethnicity. Hispanic/Latino students had higher cumulative EI scores than their peers, well above the study’s mean EI score. American Indian/Alaska Native respondents also scored well above the mean. Asian respondents scored well below the mean. These data points present some important points to consider. A previous study of Asian school teachers using similar EI measurement methods found their overall EI mean score to be 122.15.21 Compared to the Asian students in this study, there is a significant deficit. This is problematic as medical professionals are asked to practice in emotionally charged situations every day. They deal with difficult situations, provide important care, and need to be emotionally intelligent to do so effectively. If individuals entering medical professions already exhibit lower levels of emotional intelligence compared to their counterparts, and studies indicate that their emotional intelligence further declines after graduation, it suggests that the medical field may face even greater challenges in this regard than the education sector. On a broader scale, intuition would suggest that one’s upbringing, culture, and lived experiences, in part due to their race and ethnicity, are contributory to overall EI. Emotional intelligence may also mean different things to different people groups with different ethnic and cultural backgrounds. That being said, the foundational underpinning of EI’s relationship to race and ethnicity is unclear. However, these findings are clear in one sense; EI education needs to include cultural competencies and ethnic considerations for maximum effectiveness.
Limitations and Future Research
As with every research study, this study was partially limited in scope. Relatively small sample sizes existed in the racial/ethnic subgroups, despite significant results. However, in an effort to continue the important investigation of EI’s association with race and ethnicity, future research could utilize a larger scale. Incongruence amongst the male and female populations (8 males and 31 females) was also a limiting consideration in results. More robust study is warranted to investigate the origins and associations between gender and overall EI. Additionally, this study served as a snapshot view of EI. Further research is warranted in a longitudinal manner to evaluate EI over the entire course of an educational program, as curricula advances and trainees grow. These suggestions could provide valuable insight on EI development throughout the health care training process and into the transition to clinical practice.
Conclusions
Medical professionals routinely engage in stressful, demanding situations. They interact with diverse populations, provide nuanced care, and are called to communicate to patients with empathy. Their jobs can be difficult and are often emotionally taxing. Proficiency in emotional intelligence has been shown to improve patient and provider quality of life on a number of fronts. It would make sense, then, for these practitioners to receive a significant amount of time learning about EI and being trained on how to use it in a clinical setting. More emphasis should be placed on EI during the admissions process and curriculum of medical and other allied health graduate programs. It should be implemented in a culturally competent manner, considering racial and ethnic variables. If these ideals were made reality, healthcare students would be more adept at meeting their patients’ unique needs in a variety of settings.
References
1. Hally. A brief history of IQ tests. Pridobljeno. https://www.researchgate.net/profile/Thomas-Hally/publication/275354727_A_Brief_History_of_IQ_Tests/links/553ad9720cf29b5ee4b652be/A-Brief-History-of-IQ-Tests.pdf
2. Wagner RK. Intelligence, training, and employment. Am Psychol. 1997;52(10):1059-1069.
3. Schutte NS, Malouff JM, Hall LE, et al. Development and validation of a measure of emotional intelligence. Pers Individ Dif. 1998;25(2):167-177.
4. Conte JM. A review and critique of emotional intelligence measures. J Organ Behav. 2005;26(4):433-440.
5. Konrath SH, O’Brien EH, Hsing C. Changes in dispositional empathy in American college students over time: a meta-analysis. Pers Soc Psychol Rev. 2011;15(2):180-198.
6. Bosch B, Mansell H. Interprofessional collaboration in health care: Lessons to be learned from competitive sports. Can Pharm J . 2015;148(4):176-179.
7. Barello S, Graffigna G. Patient engagement in healthcare: pathways for effective medical decision making. Neuropsychol trends. 2015;(17):53-65.
8. Cadman C, Brewer J. Emotional intelligence: a vital prerequisite for recruitment in nursing. J Nurs Manag. 2001;9(6):321-324.
9. Herbert R, Edgar L. Emotional intelligence: a primal dimension of nursing leadership? Nurs Leadersh . 2004;17(4):56-63.
10. Lewis N, Rees C, Hudson N. Helping medical students identify their emotional intelligence. Med Educ. 2004;38(5):563.
11. Freshwater D. Impact of emotional abuse on the individual. J Psychiatr Ment Health Nurs. 2004;11(5):505-507.
12. Pérez-Fuentes MDC, Molero Jurado MDM, Gázquez Linares JJ, Oropesa Ruiz NF. The Role of Emotional Intelligence in Engagement in Nurses. Int J Environ Res Public Health. 2018;15(9). doi:10.3390/ijerph15091915
13. Stratton TD, Elam CL, Murphy-Spencer AE, Quinlivan SL. Emotional Intelligence and Clinical Skills: Preliminary Results from a Comprehensive Clinical Performance Examination. Academic Medicine. 2005;80(Supplement):S34-S37. doi:10.1097/00001888-200510001-00012
14. Schutte NS, Malouff JM, Hall LE, et al. Development and validation of a measure of emotional intelligence. Pers Individ Dif. 1998;25(2):167-177.
15. Zhoc KCH, Li JCH, Webster BJ. New Reliability and Validity Evidence of the Emotional Intelligence Scale. J Psychoeduc Assess. 2017;35(6):599-614.
16. Hildebrand RA, Volberding J, Carr WD. Examining Emotional Intelligence Differences in Athletic Training Undergraduate Students and First-Year Graduate Assistants. Journal of the Oklahoma Association for Health, Physical Education, Recreation and Dance. 2012;49(1):47.
17. Volberding JL, Baghurst T, Brown TC. Emotional intelligence levels of undergraduate kinesiology students: Brief report. N Am J Psychol. 2015;17(1):37-44.
18. Bar-On R, Brown JM, Kirkcaldy BD, Thomé EP. Emotional expression and implications for occupational stress; an application of the Emotional Quotient Inventory (EQ-i). Pers Individ Dif. 2000;28(6):1107-1118.
19. Barrett LF, Lane RD, Sechrest L, Schwartz GE. Sex Differences in Emotional Awareness. Pers Soc Psychol Bull. 2000;26(9):1027-1035.
20. Keeley C. Conscious competence model and medicine. Foot Ankle Surg. 2021;1(3):100053.
21. Chan DW. Perceived emotional intelligence and self-efficacy among Chinese secondary school teachers in Hong Kong. Pers Individ Dif. 2004;36(8):1781-1795.