Prashant Kaushik, M.D., Primary Contact Chief of Rheumatology, Northeastern Health System, Tahlequah, OK; Associate Program Director, Internal Medicine Residency Program, TMG/OMECO at NHS, Tahlequah, OK; Clinical Professor of Medicine, OSU CHS Cherokee Nation, Tahlequah, Oklahoma, USA., prashant.kaushik@okstate.edu
Anand N. Malaviya, M.D., Former Head of the Department of Medicine, and Chief of Clinical Immunology and Rheumatology Services, All-India Institute of Medical Sciences, New Delhi; Consultant Rheumatologist, 'A&R Clinic' and Visiting Sr. Consultant Rheumatologist ISIC Superspeciality Hospital, New Delhi., anand.malaviya@yahoo.com
Introduction
Epidemiological studies in the general population around the world have shown that back pain is the most common musculoskeletal (MSK) symptom.1 It is said to affect at least 40% of the adult population of the world in their lifetime, giving an approximate figure of over half a billion persons in the world having back pain in the year 2020.1 Many of the most common causes of back pain, discussed below, are initially triaged by primary care physicians; therefore, it is important to have a working knowledge of the different types of back pain and when they require consultation with other specialties.
Anatomy
The spine is the largest and most important structure in the musculoskeletal system. It is said that the phenotype of vertebrates mainly depends on the anatomy of their spine.2 Thus, humans have a particular phenotype because our spine supports standing on two legs (bipeds) instead of quadrupeds who cannot stand on two legs. It is also a fact that Homo sapiens have a particular body shape, which is largely due to the specific anatomical structure of our spine.2
Moreover, the spine shows a certain glaring paradox. It is very strong to be able to bear the body weight while standing upright; yet, its flexibility allows free movement, bending, and twisting.2 Despite such flexibility, it is designed to protect the delicate and vital spinal cord and its major nerves which connect the brain with the rest of your body making it possible to control the body movements.3 Therefore, it becomes important to understand its anatomy that provides such strength in the face of remarkable flexibility. The strong muscles, bones, and cartilage with flexible ligaments and muscles in the area make the spine such an ingenious structure. This complexity of its anatomy and physiology makes it susceptible to sprain, strain, injury, and certain diseases that are characterized by back pain.
Of course, it is not the aim of this paper to describe the detailed anatomy, mechanics, and physiology of the spine except to name some of the important structures that should be kept in mind with reference to spinal complaints/diseases.
a. The spine consists of 33 vertebrae divided into 5 distinct areas stacked over each other with ‘cushion-like’ spongy vertebral discs (vide infra).
i. Cervical spine with 7 vertebrae in the neck that support the head.
ii. Thoracic (or dorsal) spine with 12 vertebrae.
iii. Lumbar spine consists of 5 vertebrae; a main component of the ‘lower back’.
iv. Sacrum consists of 5 fused (in adults) sacral vertebrae.
v. Coccyx that (usually) consists of 4 fused (in adults) coccygeal vertebrae (the number of coccygeal vertebrae can vary from 3 to 5).
b. The intervertebral discs are made of an external ring-like structure that consists of fibrous cartilage, a highly resilient structure that can withstand high physical forces and act as shock absorbers. It is lined by the annulus fibrosus that encases a gelatinous core called the nucleus pulposus.
c. The ligaments are robust fibrous bands that hold the vertebrae in proper alignment, stabilize the spine, and shield the discs. The four major ligaments of the spine include:
i. Anterior and posterior longitudinal ligaments (ALL and PLL) that join and hold the vertebral bodies and are the two primary spine stabilizer ligaments.
ii. Supraspinous ligament that connects the tips of the vertebral spine.
iii. The interspinous ligament is a thin and short structure that attaches to another ligament called the ligamentum flavum.
iv. Ligamentum flavum that connects the laminae (a thin plate of bone that makes the roof of the vertebral canal) of adjacent vertebrae. It is the strongest ligament in the spine traversing the length of the spine from the base of the skull to the pelvis. Its main role is the protection of the spinal cord and nerves. Posteriorly, it touches the facet joint capsules.
d. Several muscles help with spinal movements. They are covered with fascia which taper off making tendons which attach to the bone. In the thoracic region, the spinal muscles are:
i. Longissimus thoracis that helps thoracic spinal extension and lateral flexion as well as rib rotation.
ii. Iliocostalis thoracis that aids in the function of longissimus thoracis.
iii. Spinalis thoracis which is the main muscle for extending the thoracic spine.
In the lumbar region:
iv. Psoas major flexes the spine at the lumbar and lower levels and at the hip joint.
v. Quadratus lumborum causes lateral flexion of the spine.
vi. Multifidus is the strongest muscle in the spine consisting of short triangular muscles that make the deep back muscle in the transversospinal group on either side of the vertebral column from the cervical to the lumbar spine.
e. The lumbar zygapophyseal joints form part of the postero-lateral element of the spinal column. These are the only synovial joints in the spine that are deeply involved in load transmission and are prone to degenerative (osteoarthritic) joint disease.3 Their involvement in inflammatory joint diseases, or other types of inflammatory arthritis including crystal arthropathies, is not well described.
Categories of back pain
Akin to joint diseases (and other diseases in the MSK system) back pain can also be classified into two common categories namely: 1. Noninflammatory, and 2. Inflammatory back pain.
Noninflammatory back pain
At the community level, noninflammatory back pain outnumbers inflammatory back pain by about 9 to 1; the former is variably reported to be stress-strain-sprain-related mechanical-structural back pain.4 As mentioned above in the anatomy section, the lumbosacral region of the spine has one of the most complex anatomies which permits flexibility yet has strength to bear heavy weights. Anatomically it includes intervertebral discs, muscles, fascia, bone, facet joints including the capsule, sacroiliac joints, symphysis pubis, and ligaments. Consequently, each of these tissues is naturally prone to mechanical-structural stress which can cause back pain.5 Yet, it is neither possible nor necessary to confirm which specific tissue is generating the back pain. An important feature of this type of back pain is that even advanced and newer methods of imaging (e.g., magnetic resonance imaging (MRI) and computed tomographic {CT} scan) do not reveal any anatomical damage in the majority of the patients that could explain the symptoms of back pain.6 Therefore, unless there are definite physical signs of progressive neurological symptoms over days (vide infra), or the patient has signs of ‘red flag’ back pain (vide infra), there is a strong recommendation against any type of imaging in such patients.6 The majority of these patients recover within days or weeks with appropriate rest and exercise under the direct guidance of physiotherapists and experts in physical medicine.7,8 It needs to be emphasized that authorities strongly advise against prolonged rest for such patients with minimum use of ‘painkillers’ and strong recommendations for encouraging early mobilization towards locomotion and return to normal life.9
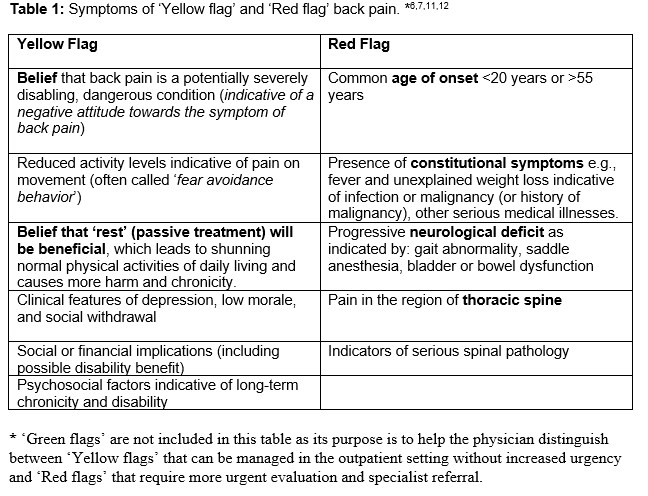
This category of nonspecific back pain is often labeled ‘Green Flag’ back pain indicating that such back pain has a good prognosis with minimum investigations and minimum use of pain-relieving drugs or any surgical interventions.9 This large category of back pain is commonly identified as nonspecific back pain meaning that a specific pathoanatomical cause explaining pain or disability cannot be identified. Therefore, as already mentioned vide supra, there is strong recommendation against any type of imaging in such patients, which would be a waste of resources without adding towards diagnosis or management.6 It needs to be mentioned here that in this category of patients with back pain, the majority would recover within 3 months. However, some would have a tendency for chronicity of back pain (persisting beyond 3 months) due to factors like ‘somatization of symptoms’, disability, and nociceptive pain.7,10 They have certain underlying neuropsychiatric personality traits that make them prone to develop chronic back pain. They are highly prone to become dependent on painkillers of different types. Such patients are often labeled as having ‘Yellow Flag’ back pain (see Table 1).7 Such patients are strongly encouraged to resume normal activities as soon as possible explaining that this will help to relieve symptoms and reduce the risk of chronic disability. However, some of them may require help from a ‘pain management team’ including psychiatric help.
It is of note that in the ‘noninflammatory back pain’ category (vide supra) there is a subcategory of a small number of patients that can have ‘red flag’ back pain. ‘Red flags’ are possible indicators of serious spinal pathology (e.g., malignancy, infection, fracture, or severe neurologic compromise) which require urgent consultation with specialized spinal surgeons (see Table 1).6,11,12
Inflammatory back pain
Certain specific features in clinical assessment of back pain easily identify inflammatory back pain. Thus, back pain of (i) >3 months duration, (ii) onset before the age of 45 years, (iii) associated with stiffness after a period of immobility that takes > 30’ of gentle movements to start improving, and (iv) good response to nonsteroidal anti-inflammatory drugs (NSAIDS including nonselective {COX 1 and 2} and selective {COX 2 inhibitors}), are time-honored clinical features of inflammatory back pain, yet not infallible.9 These features serve as a ‘screening’ method for a quick categorization in ‘inflammatory’ and distinguishing it from ’non-inflammatory’ categories of back pain that further requires erythrocyte sedimentation rate (ESR) and c-reactive protein (CRP) levels to confirm the inflammatory nature.11 This broad category of inflammatory back pain has been given a generic name spondyloarthritis (SpA).13
There is a subcategory of SpA that has an inherent tendency to rapid progression involving the ligaments that hold individual vertebrae together; they become rigid with calcification (visible on plain radiograph of the spine identified as syndesmophytes) making the spine immobile and rigid. Such spinal changes are called the ‘bamboo spine’. This stage of SpA is a well-defined specific subcategory of SpA given the name ‘ankylosing spondylitis’ (AS). It should be clearly understood that only a minority of patients with SpA who progress to the stage of AS.13 Further, a combination of human leukocyte antigen (HLA) B27 positivity and severe sacroiliitis has demonstrated a high specificity for the development of AS in patients with early inflammatory back pain.14 Regardless of SpA severity, a Rheumatology referral is warranted, and the international guidelines for treatment outlined by the Assessment of SpondyloArthritis International Society (ASAS)-EULAR should be followed.15
Conclusion:
Back pain is one of the most common musculoskeletal symptoms in clinical practice. Therefore, clinically classifying such patients into two main categories namely: 1. ‘Noninflammatory’ and 2. ‘Inflammatory’ back pain, helps in their triaging. Thus, most patients with noninflammatory back pain with ‘green flag’ features can be treated by primary care physicians or referred to the Department of ‘Physical Medicine & Rehabilitation’. The majority of them recover within days, weeks, or at the most within 3 months of the onset with physical medicine help and minimal rest and painkillers. If the ‘green flag’ back pain gets prolonged beyond 3 months becoming a ‘yellow flag’, then the patient must be referred to ‘Pain Management’. If there are clinical features of ‘red flag’ back pain, such as saddle anesthesia or loss of bowel or bladder, a spinal surgeon must get involved in their management right from the outset. However, if the patient has clinical features of ‘inflammatory’ back pain, the patient must be evaluated by rheumatology to confirm the diagnosis of spondyloarthritis and appropriate treatment according to the international guidelines, as soon as possible before permanent damage develops.
References:
1. The Lancet Rheumatology. The global epidemic of low back pain. Lancet Rheumatol. 2023 Jun;5(6):e305. doi: 10.1016/S2665-9913(23)00133-9. PMID: 38251593.
2. Boszczyk, B.M., Boszczyk, A.A. and Putz, R. (2001), Comparative and functional anatomy of the mammalian lumbar spine. Anat. Rec., 264: 157-168. https://doi.org/10.1002/ar.1156
3. Edelle Carmen Field-Fote, Spinal Cord Control of Movement: Implications for Locomotor Rehabilitation Following Spinal Cord Injury, Physical Therapy, Volume 80, Issue 5, 1 May 2000, Pages 477–484, https://doi.org/10.1093/ptj/80.5.477
4. Burgos-Vargas, R., & Braun, J. (2012). Inflammatory back pain. Rheumatic diseases clinics of North America, 38 3, 487-99 . doi.org/10.1016/j.rdc.2012.08.014
5. Borenstein, D. Mechanical low back pain—a rheumatologist's view. Nat Rev Rheumatol 9, 643–653 (2013). https://doi.org/10.1038/nrrheum.2013.133
6. Chiarotto A, Koes BW. Nonspecific Low Back Pain. N Engl J Med. 2022 May 5;386(18):1732-1740. doi: 10.1056/NEJMcp2032396. PMID: 35507483.
7. Ashar YK, Gordon A, Schubiner H, Uipi C, Knight K, Anderson Z, et al. Effect of Pain Reprocessing Therapy vs Placebo and usual care for patients With Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry. 2022 Jan 1;79(1):13-23. doi: 10.1001/jamapsychiatry.2021.2669. PMID: 34586357; PMCID: PMC8482298.
8. Cohen KR. Management of Chronic Low Back Pain. JAMA Intern Med. 2022 Feb 1;182(2):222-223. doi: 10.1001/jamainternmed.2021.7359. PMID: 34928311.
9. Traeger AC, Qaseem A, McAuley JH. Low Back Pain. JAMA. 2021 Jul 20;326(3):286. doi: 10.1001/jama.2020.19715. PMID: 34283182.
10. Stevans JM, Delitto A, Khoja SS, Patterson CG, Smith CN, Schneider MJ, et al. Risk Factors Associated With Transition From Acute to Chronic Low Back Pain in US Patients Seeking Primary Care. JAMA Netw Open. 2021 Feb 1;4(2):e2037371. doi: 10.1001/jamanetworkopen.2020.37371. PMID: 33591367; PMCID: PMC7887659.
11. Grinnell-Merrick LL, Lydon EJ, Mixon AM, Saalfeld W. Evaluating Inflammatory Versus Mechanical Back Pain in Individuals with Psoriatic Arthritis: A Review of the Literature. Rheumatol Ther. 2020 Dec;7(4):667-684. doi: 10.1007/s40744-020-00234-3. Epub 2020 Sep 15. PMID: 32935330; PMCID: PMC7695767.
12. Lancaster B, Goldman J, Kobayashi Y, Gottschalk AW. When Is Imaging Appropriate for a Patient With Low Back Pain?. Ochsner J. 2020;20(3):248-249. doi:10.31486/toj.20.0077
13. van der Heijde D, Ramiro S, Landewé R, Baraliakos X, Van den Bosch F, Sepriano A, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017 Jun;76(6):978-991. doi: 10.1136/annrheumdis-2016-210770. Epub 2017 Jan 13. PMID: 28087505.
14. Bennett AN, McGonagle D, O’Connor P, et al. Severity of baseline magnetic resonance imaging-evident sacroiliitis and HLA-B27 status in early inflammatory back pain predict radiographically evident ankylosing spondylitis at eight years, Arthritis Rheum. 2008;58:3413-8
15. Ramiro S, Nikiphorou E, Sepriano A, et alASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann Rheum Dis. 2023;82:19-34.