SDOH and Poor Mental Health Days
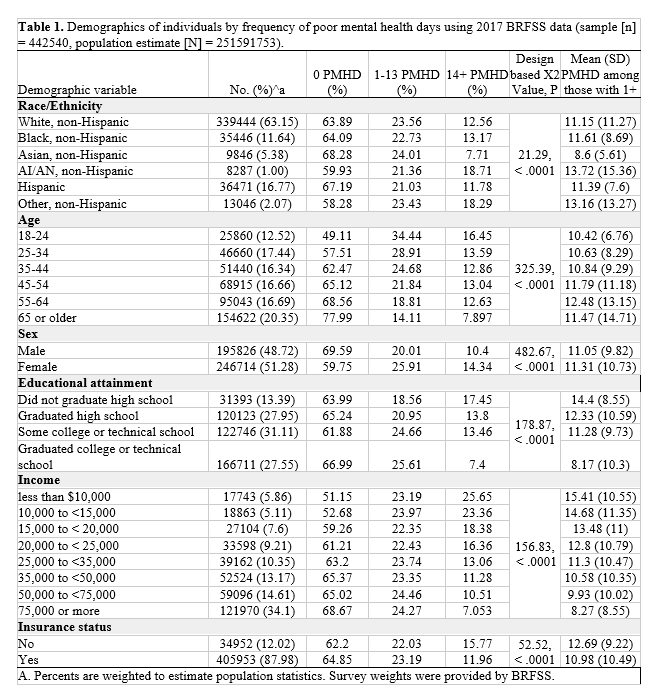
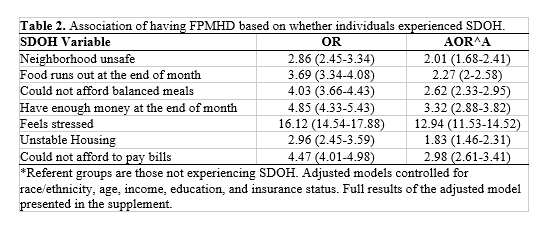
The analysis revealed that individuals who experienced SDOH were more likely to have FPMHD compared to those who did not experience SDOH. Specifically, individuals who reported living in an unsafe neighborhood had 2.86 times greater odds of having FPMHD (95% CI: 2.45-3.34), which decreased to 2.01 (95% CI: 1.68-2.41) after adjusting for race/ethnicity, age, income, education, and insurance status. Similarly, individuals who reported running out of food at the end of the month had a 2.27 (95% CI: 2.00-2.58) times greater adjusted odds of having FPMHD. Individuals who reported not being able to afford balanced meals and not having enough money at the end of the month also had a significantly higher odds of having FPMHD (AOR: 2.62; 95% CI: 2.33-2.95, and 3.32; 95% CI: 2.88-3.82, respectively) compared to individuals not experiencing these domains. Similar results were found among those with unstable housing and inability to pay bills. The association between feeling stressed and FPMHD was the strongest among all the SDOH variables examined—with the adjusted model estimating an AOR of 12.94 (95% CI: 11.53-14.52). The full multivariable regression results are included in supplement 1.
Poor Mental Health Days by State
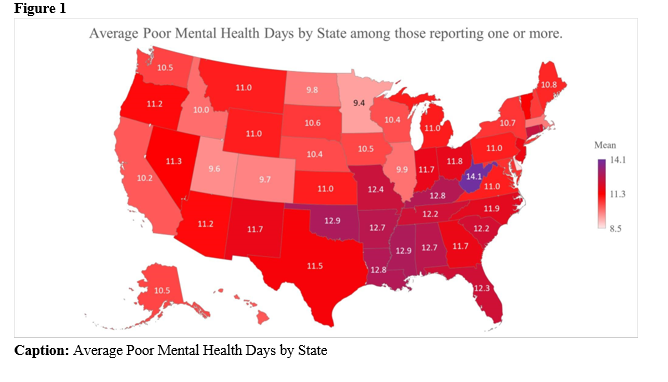
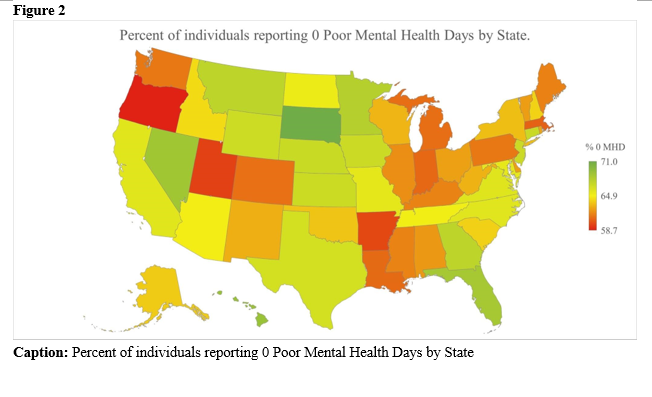
All states report greater than 50% of their population experiencing 0 poor mental health days per month. Individuals reporting the most frequent 0 poor mental health days per month were South Dakota, (70.99%; Figure 1), Hawaii (69.08%), and Nevada (68.70%). States reporting the least frequency of 0 poor mental health days per month were Oregon (58.7%), Utah (59.65%), and Arkansas (59.84%). Although over 60% of individuals from West Virginia, Oklahoma, and Mississippi reported 0 PMHD per month, those that did experience PMHD reported the highest average number of PMHD per month compared to any other state with 14.11 days, 12.94 days, and 12.87 days, respectively (Figure 2). States with the lowest average number of PMHD per month were Delaware (8.65 days) and Minnesota (9.38 days).
Discussion
With persistent disparities in mental health care and a growing burden of mental health disease, this study investigated the frequency of PMHD and SDOH by race, age group, SES, and sex. We found a statistically significant association between FPMHD and all SDOH variables as well as disparities in reporting on FPMHD based on race, gender and age. State differences in reported FPMHD were also identified. States with the highest rates of individuals reporting 0 poor mental health days per month were South Dakota, Hawaii, and Nevada, while those with the lowest rates of reporting 0 poor mental health days were Oregon, Utah, and Arkansas. Among individuals reporting at least 1 poor mental health day, the states with the highest average number of PMHD per month were West Virginia, Oklahoma, and Mississippi. These findings highlight the growing need to address gaps in mental health care resources across the U.S.
Mental health has been shown to negatively affect overall health. For example, individuals experiencing depression are at a higher risk for developing physical illnesses.32 One study found that mental health both directly and indirectly — via lifestyle choices and social interactions — influences physical health.33 It has been shown that poverty is associated with an increased prevalence of mental health disorders.34 Additionally, individuals living in low SES neighborhoods have shown to have increased stressors, fewer resources, and fewer support sources which increases their risk of having poor mental health.34 Meyer et al., demonstrated that low SES was associated with increased concerns regarding neighborhood safety causing a negative association with physical activity and leading to worsened mental and self-rated health.20 All of these findings are in agreement with our findings of FPMHD being significantly associated with SDOH domains with the stress domain being the most notably significant. Interestingly, Mississippi, West Virginia, and Oklahoma are all rated within the top 10 most stressed states in the US35, and individuals in these states reported the highest average number PMHD per month. Therefore, exploring factors that may be influencing regional differences in FPMHD might highlight areas for improvement within these states.
All states reported greater than 50% of their population experiencing 0 PMHD. However, state differences existed between the populations who reported experiencing PMHD. Individuals living in Minnesota and Delaware had the lowest average number of PMHD reported compared to all states. According to the 2022 Mental Health America report, Minnesota consistently landed in the top 13 states for lowest prevalence of mental health illness and highest rates of access to mental health care resources.36 Additionally, the 2022 United Health Foundation found that in Minnesota and Delaware, the number of licensed mental health practitioners were 320 and 317 per 100,000 respectively, compared to a US average of only 305 per 100,000.37 These higher average numbers of mental health providers may account for increased access to mental health services in these states and thus, the lower average number of PMHD. However, to maintain adequate access to mental health services, state governments in both Minnesota and Delaware must continue to identify areas of weakness in mental health resources for continued provision of adequate mental health care and to maintain low FPMHD among their population.
Conversely, West Virginia, Oklahoma and Mississippi were found to have the highest reported FPMHD. The 2022 United Health Foundation (UHF) found West Virginia and Mississippi had a much lower number of licensed mental health practitioners per capita (165 and 205 per 100,000 residents, respectively). 37 However despite Oklahoma being one of the states with the highest reported rate of FPMHD, the UHF found their per capita rate of mental health practitioners to be 424 per 100,000 residents, which is above the national average of 305. Conversely, a study by Andrilla et al., using the 2015 National Provider Identification data to assess for regional differences in per capita supply of psychiatrists, psychologists, and psychiatric nurse practitioners found that the West South Central Census Division, which includes Oklahoma, had among the lowest supply of all three provider types with a total of 26 per 100,000, while the national average was 47 per 100,000 with larger deviations among non-metropolitan areas.38 This variation in reported estimates of mental health practitioner shows that Oklahoma has made efforts to increase its supply of mental health practitioners in the last 7 years, however, FPMHD continues to be high in the state highlighting the fact that other barriers to accessing mental health services may continue to exist. Therefore, to address these disparities, states must identify barriers to mental health care and avenues for improvement in order to decrease FPMHD.
Recommendations
Identifying barriers to mental health care implementation would be the first step in improving outcomes. Currently, there is an identified national shortage of mental health care providers by the Association of American Medical Colleges with more than half of U.S. counties lacking a single psychiatrist in 2018.39,40 Additionally, telehealth measures continue to lag behind need due to unreliable or limited broadband or cellular service access in rural communities, and concerns about data security and patient privacy.41,42 Both of which limit the reach and utility of virtual telehealth services as a tool for increasing access to care. Some potential recommendations, especially in rural and urban underserved areas could be the use of faith based mental health resources.43,44 By incorporating mental health care into trusted community centers such as churches, individuals with increased burden of mental health illness might be more aptly reached. Another possible community intervention could be the use of library systems to reach those in need of mental health care. The addition of mental health services to library systems could take the form of lectures for the public, training programs for library staff, a directory of readily available community health resources and referrals for patrons who have mental health conditions.45 An additional focus should be placed on ensuring community based interventions to improve mental health are evidence-based and include specific recommendations for neurodiverse populations.
A model that has been adopted by Oklahoma in 2016 to increase access to mental healthcare is the Project Extension for Community Health Care Outcomes (ECHO) model46 which shows some institutions are initiating systems to improve mental health services within the state. Project ECHO expands access to preventive and specialty care for rural and underserved urban populations by building the capacity of primary care physicians and community health workers.47 Osei-Twum et al., conducted a scoping review of 15 studies describing Project ECHO programs to examine the impact of Project ECHO programs on patient and community health outcomes.48 They identified emerging evidence of the effectiveness of Project ECHO as a tele-education model that improves patient health outcomes and may potentially improve community health.48
Limitations and Future Research
Limitations to our study include that all data was self-reported via survey which increases the risk for recall bias. However, BRFSS is a nationally recognized survey completing over 400,000 interviews every year which makes it the largest survey system in the world.49 Additionally, our study is cross-sectional in nature, therefore our results should be interpreted as correlational rather than causal. Individuals experiencing SDOH and increased FPMHD have shown to experience all domains of SDOH including decreased access to care, affordability, and increased stress. Looking forward, future research should focus on further implementation of resources such as project Echo, telehealth, or community-based interventions to increase access to mental health care services which may lead to improvement in mental health outcomes, thus decreasing FPMHD and improving overall health.
Conclusion
Our study highlights the impact of social determinants of health on mental health, revealing differences in frequency of poor mental health days among those who have and do not have access to resources. We also found variations in the rates of poor mental health days by states—with the highest average number found in West Virginia, Oklahoma, and Mississippi—coinciding with states with the greatest shortages of mental health practitioners. While some institutions in these states are making efforts to improve access to mental health services, they still face significant challenges. Therefore, expanded mental health care through improved medical coverage for mental health services, and increased numbers of evidence-based programs and community-based centers for mental health, may improve the mental health of individuals experiencing increased domains of SDOH.
Disclosure Statement: Dr. Hartwell receives funding from the Human Resources Services Administration for research (U4AMC44250-01-02, PI: Audra Haney; R41MC45951 PI: Hartwell).
Role of Funding Source: This study was not funded.
References
1. Twenge JM, Gentile B, DeWall CN, Ma D, Lacefield K, Schurtz DR. Birth cohort increases in psychopathology among young Americans, 1938-2007: A cross-temporal meta-analysis of the MMPI. Clin Psychol Rev. 2010;30(2):145-154.
2. Mental health: strengthening our response. Accessed May 24, 2022. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
3. Ahola K, Virtanen M, Honkonen T, Isometsä E, Aromaa A, Lönnqvist J. Common mental disorders and subsequent work disability: a population-based Health 2000 Study. J Affect Disord. 2011;134(1-3):365-372.
4. Stansfeld S, Feeney A, Head J, Canner R, North F, Marmot M. Sickness absence for psychiatric illness: the Whitehall II Study. Soc Sci Med. 1995;40(2):189-197.
5. Mental Illness. National Institute of Mental Health (NIMH). Accessed October 1, 2022. https://www.nimh.nih.gov/health/statistics/mental-illness
6. Mental Health By the Numbers. Accessed October 1, 2022. https://www.nami.org/mhstats
7. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137-150.
8. Poor Mental Health Days. County Health Rankings & Roadmaps. Accessed October 11, 2022. https://www.countyhealthrankings.org/explore-health-rankings/measures-data-sources/county-health-rankings-model/health-outcomes/quality-of-life/poor-mental-health-days
9. Jessica Allen (Medical policy specialist), Marmot M. Social Determinants of Mental Health.; 2014.
10. Gruebner O, Rapp MA, Adli M, Kluge U, Galea S, Heinz A. Cities and Mental Health. Dtsch Arztebl Int. 2017;114(8):121-127.
11. Marmot M, Commission on Social Determinants of Health. Achieving health equity: from root causes to fair outcomes. Lancet. 2007;370(9593):1153-1163.
12. Social determinants of health. Accessed October 3, 2022. https://health.gov/healthypeople/priority-areas/social-determinants-health
13. Bush M. Addressing the Root Cause: Rising Health Care Costs and Social Determinants of Health. N C Med J. 2018;79(1):26-29.
14. 14. Wang J, Geng L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. Int J Environ Res Public Health. 2019;16(2). doi:10.3390/ijerph16020281
15. Safran MA, Mays RA Jr, Huang LN, et al. Mental health disparities. Am J Public Health. 2009;99(11):1962-1966.
16. Reiss F, Meyrose AK, Otto C, Lampert T, Klasen F, Ravens-Sieberer U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: Results of the German BELLA cohort-study. PLoS One. 2019;14(3):e0213700.
17. Edwards VJ, Anderson LA, Thompson WW, Deokar AJ. Mental health differences between men and women caregivers, BRFSS 2009. J Women Aging. 2017;29(5):385-391.
18. Paradies Y, Ben J, Denson N, et al. Racism as a Determinant of Health: A Systematic Review and Meta-Analysis. PLoS One. 2015;10(9):e0138511.
19. Mental Health Disparities: Diverse Populations. Accessed November 8, 2024. https://www.psychiatry.org:443/psychiatrists/diversity/education/mental-health-facts
20. Meyer OL, Castro-Schilo L, Aguilar-Gaxiola S. Determinants of mental health and self-rated health: a model of socioeconomic status, neighborhood safety, and physical activity. Am J Public Health. 2014;104(9):1734-1741.
21. Rapp MA, Kluge U, Penka S, et al. When local poverty is more important than your income: Mental health in minorities in inner cities. World Psychiatry. 2015;14(2):249-250.
23. Iceland J, Sharp G. White Residential Segregation in U.S. Metropolitan Areas: Conceptual Issues, Patterns, and Trends from the US Census, 1980 to 2010. Popul Res Policy Rev. 2013;32(5). doi:10.1007/s11113-013-9277-6
24. Acs G, Pendall R, Treskon M, Khare A. The Cost of Segregation: National Trends and the Case of Chicago, 1990–2010. Published online March 27, 2017. Accessed October 12, 2022. https://policycommons.net/artifacts/631635/the-cost-of-segregation/1612940/
25. Fone D, White J, Farewell D, et al. Effect of neighbourhood deprivation and social cohesion on mental health inequality: a multilevel population-based longitudinal study. Psychol Med. 2014;44(11):2449-2460.
26. Honold J, Wippert PM, van der Meer E. Urban Health Resources: Physical and Social Constitutes of Neighborhood Social Capital. Procedia - Social and Behavioral Sciences.2014;131:491-496. doi:10.1016/j.sbspro.2014.04.154
27. Miller CE, Vasan RS. The southern rural health and mortality penalty: A review of regional health inequities in the United States. Soc Sci Med. 2021;268:113443.
28. James W, Cossman J, Wolf J. Persistence of death in the United States: The remarkably different mortality patterns between America’s Heartland and Dixieland. Demographic Research. 2018;39:897-910. doi:10.4054/demres.2018.39.33
29. Olfson M. The Rise of Primary Care Physicians in the Provision of US Mental Health Care. J Health Polit Policy Law. 2016;41(4):559-583.
30. Cherry D, Albert M, McCaig LF. Mental Health-related Physician Office Visits by Adults Aged 18 and Over: United States, 2012-2014. NCHS Data Brief. 2018;(311):1-8.
31. About BRFSS. February 9, 2019. Accessed October 13, 2022. https://www.cdc.gov/brfss/about/index.htm
32. Chronic Illness and Mental Health: Recognizing and Treating Depression. National Institute of Mental Health (NIMH). Accessed March 12, 2023. https://www.nimh.nih.gov/health/publications/chronic-illness-mental-health
33. Ohrnberger J, Fichera E, Sutton M. The relationship between physical and mental health: A mediation analysis. Soc Sci Med. 2017;195:42-49.
34. Lund C, Brooke-Sumner C, Baingana F, et al. Social determinants of mental disorders and the Sustainable Development Goals: a systematic review of reviews. Lancet Psychiatry. 2018;5(4):357-369.
35. Moya MJ. People in these US states are the most stressed, report finds. USA Today. https://www.usatoday.com/story/news/nation/2022/03/29/most-stressed-us-states/7201723001/. March 29, 2022. Accessed March 13, 2023.
36. Reinert, M, Fritze, D. & Nguyen, T. The State of Mental Health in America 2022. Published online October 2021. Accessed February 17, 2023. https://mhanational.org/sites/default/files/2022%20State%20of%20Mental%20Health%20in%20America.pdf
37. America’s Health Rankings. America’s Health Rankings. Accessed February 26, 2023. https://www.americashealthrankings.org/explore/annual/measure/MHP/state/DE?edition-year=2022
38. Andrilla CHA, Patterson DG, Garberson LA, Coulthard C, Larson EH. Geographic Variation in the Supply of Selected Behavioral Health Providers. Am J Prev Med. 2018;54(6):S199-S207.
39. Weiner S. A growing psychiatrist shortage and an enormous demand for mental health services. AAMC. August 9, 2022. Accessed March 13, 2023. https://www.aamc.org/news-insights/growing-psychiatrist-shortage-enormous-demand-mental-health-services
40. 40. Angela J. Beck, PhD, MPH Cory Page, MPH, MPP Jessica Buche, MPH, MA Danielle Rittman Maria Gaiser. Estimating the Distribution of the U.S. Psychiatric Subspecialist Workforce. Behavioral Health Workforce. 2018. Accessed March 13, 2023. https://behavioralhealthworkforce.org/wp-content/uploads/2019/02/Y3-FA2-P2-Psych-Sub_Full-Report-FINAL2.19.2019.pdf
41. Blandford A, Wesson J, Amalberti R, AlHazme R, Allwihan R. Opportunities and challenges for telehealth within, and beyond, a pandemic. The Lancet Global Health. 2020;8(11):e1364-e1365.
42. Democratizing access to and understanding of health information in the era of telehealth. In: Diabetes Digital Health and Telehealth. Academic Press; 2022:3-13.
43. Blank MB, Mahmood M, Fox JC, Guterbock T. Alternative mental health services: the role of the black church in the South. Am J Public Health. 2002;92(10):1668-1672.
44. Hankerson SH, Weissman MM. Church-based health programs for mental disorders among African Americans: a review. Psychiatr Serv. 2012;63(3):243-249.
45. Stringer H. Libraries as mental health hubs: Across the United States, libraries are striving to offer visitors mental health supports. American Psychological Association. 2020. Accessed March 13, 2023. https://www.apa.org/monitor/2020/04/libraries-health-hubs
46. Mental Health ECHO - Oklahoma State University. March 18, 2021. Accessed April 12, 2023. https://medicine.okstate.edu/echo/mental-health-echo.html
47. PROJECT ECHO®: A TELEHEALTH MODEL FOR RURAL HEALTH CARE. Oklahoma State Department of Health. August 2019. Accessed February 26, 2023. https://oklahoma.gov/content/dam/ok/en/health/health2/documents/fs-up-project-echo-2019.pdf
48. Osei-Twum JA, Wiles B, Killackey T, Mahood Q, Lalloo C, Stinson JN. Impact of Project ECHO on Patient and Community Health Outcomes: A Scoping Review. Acad Med. 2022;97(9):1393.
49. Behavioral Risk Factor Surveillence System. (2020). Data User Guide. Center for Disease Control and Prevention; 2022. Accessed September 28, 2022. https://www.cdc.gov/brfss/index.html