Perceived Stress and Coping Mechanisms Observed in Osteopathic Medical
Emily Madrak, PhD, LAT, ATC. Assistant Professor, The University of Virginia
Department of Kinesiology, Charlottesville, VA
Jennifer L. Volberding, PhD, LAT, ATC., Department Chair
Professor, Athletic Training Program Director, Oklahoma State University Center for Health Sciences School of Allied Health, Department of Athletic Training, Tulsa, OK
Emily Madrak, PhD, LAT, ATC (corresponding author)
Assistant Professor
The University of Virginia
Department of Kinesiology
322 SHWC
550 Brandon Ave
Charlottesville, VA 22903
570 877-22278 (cell)
434-924-6187 (office)
Cvy5fx@virginia.edu
Jennifer L. Volberding, PhD, LAT, ATC
Department Chair
Professor
Athletic Training Program Director
Oklahoma State University Center for Health Sciences
School of Allied Health
Department of Athletic Training
Tulsa, OK 74107
Funding: none
Disclosures: none
ABSTRACT
Background
This research investigated perceived stress (PS) in osteopathic medical students and whether selected coping skills (CS) increase or decrease PS. Additionally, the research explored which demographic groups experience higher levels amounts of PS, and the CS most often utilized by those groups. Researchers were interested in determining how these factors might affect the medical school experience.
Methods
Participants from a college of osteopathic medicine completed a survey consisting of the Perceived Stress Scale, and the Coping Orientation to Problem Experience Inventory. Perceived Stress and CS were analyzed separately using independent t-tests, Mann-Whitney tests, ANOVAs, and Kruskal-Wallis Tests. Multiple regression analyses were used to determine a potential relationship between PS and CS.
Results
Medical students experienced moderate PS, M=15.91, (SD=7.60). In terms of CS, venting and mental disengagement demonstrated increases in PS while emotional support and planning demonstrated decreases in PS. Females demonstrated greater levels in the following CS in comparison to males: PS (M=18.50, SD=7.28), males (M=13.81, SD=7.29), t(65)=2.62, p=0.01, venting, females (Mdn=10.00) males (Mdn=7), U(Nfem=30, Nmales=37)=258.00, z= -3.77, p<0.00. and emotional support, females (Mdn = 13.50) males (Mdn = 11.00), U(Nfem=30, Nmales=37)=390.50, z= -2.09, p<0.05. Males demonstrated greater coping with restraint in comparison to females, males (M=11.16, SD=2.85), females (M=9.87, SD=2.21), t(65)= -2.04, p < 0.05. Significance in CS for school years was observed with humor, X2(3)=8.20, p=0.04. Third-year students demonstrated greater use of humor as a CS than second-years, MD= -3.65, p=0.04. Multiple regression revealed increases in PS with coping skills: mental disengagement and venting, (β =0.35, t(50)=3.90, p<0.00); (β = 0.56, t(50)=5.27, p<0.00), and decreases in PS with CS emotional support (β = -0.26, t(50)= -2.28, p=0.03), and planning (β= -0.34, t(50)= -2.70, p <0.01).
Conclusion
The level of PS may be associated with greater levels of depression which may negatively impact performance in medical school and as a future professional. Maladaptive emotion-focused CS, such as venting and mental disengagement, demonstrate a relationship to increased PS, while action-oriented CS like planning demonstrate a relationship with decreased PS.
Key Words: Coping Mechanisms, Emotion-Focused Coping, Osteopathic Medical School, Perceived Stress, Problem-Focused Coping
INTRODUCTION
Stress is a sensation that humans experience daily, but despite its familiarity, how do we begin to define it?1 Stress is defined as bodily adaptations when it moves outside of homeostasis.2 Further, it is described as “the bodily tension felt when a variable alters the equilibrium of an existing object.”2 In the United States, the overall increase in stress is related to job pressure, money, health, and relationships, among others.3,4 Additionally, higher education has been touted as one of the largest contributors to stress, especially among students matriculated to medical school.4
Graduate students, in general, are known to carry large amounts of stress due to academia, finances, and other contributing factors.5 Approximately 70% of graduate students experience academic stress, with 32% of those students often neglecting their studies due to stressors outside of academia.1 When looking at graduate disciplines, medical students may experience more stress than other disciplines due to the academic rigor involved and their curriculum.6 Previous research suggests that medical school may be one of the most trying times in life and can result in significantly lower levels of quality of life.6
Most medical school curricula in the United States involves four years; two of didactic and two of clinical experiences/clerkships. The first year in medical school is known to be particularly difficult in terms of stress, marked by significant decreases in physical and mental health.7 It has been suggested that this is due to the rigor of academics and the transition period of a new environment.7 Additionally, this decline in health can be marked by the lack of an internal structure to support specific personality and temperament factors, most likely due to underdeveloped coping skills. 7These factors therefore put students at risk for burnout during these early years of medical education.7 Furthermore, this risk for burnout can contribute to improper decision making, potentially resulting in ineffective care when working with patients.8 Considering this, the researchers hypothesized first-year medical students to have an increased level of perceived stress. In order to better understand how students cope with this stress, the dimensions of coping skills require further discussion.
Coping skills are divided into two different dimensions, problem-focused coping and emotion-focuced.9 Lazarus and Folkman9 classified problem-focused coping as “attacking” the problem with intentions to gain information, alter the event, and increase awareness. The active action is dealing directly with the stressor, and these coping skills are more constructive and most often result in a more favorable outcome.10 Carver et al11 divided problem-focused coping into five different dimensions: active coping, planning, suppression, restraint, and social support. Active coping is taking a direct action in a stepwise fashion to circumvent the stressor.11 Planning is determining what the best strategy is to handle the stress; it represents a more secondary appraisal compared to active which is a primary appraisal.11 Suppression involves putting other activities or events aside in order to deal with the current stressor.11 Restraint is used in the sense of not acting prematurely and waiting until the right moment to act upon the stressor.11 Social Support can be branched into problem and emotion focused coping.11 Problem-focused social support focuses on seeking advice or assistance.11 Emotion-focused social support seeks to vent or look for sympathy; these two variations often occur concurrently.
Emotion-focused coping is a psychological change designed to prevent emotional disruption caused by an event, without altering the event itself; essentially enduring the stressor.2, 9 Carver et al11 divided emotion-focused coping into seven categories: Venting, behavioral disengagement, mental disengagement, positive reinterpretation and growth, denial, acceptance, and religious.11 The focusing on and venting of emotions requires the person to focus on whatever the stressor is and express the feelings; it may tend to be maladaptive due to the negative focus.11 Behavioral disengagement is essentially “giving up” on attaining goals that the stressor may be interfering with or lessening the effort in dealing with the stressor.11 Mental disengagement is used when behavioral disengagement is not able to be used; it entails distraction from the stressor by doing alternative activities to take the mind away from the stressor.11 Positive reinterpretation and growth are focusing on the emotions rather than the stressor and aids in transitioning to problem-focused coping.11 Denial is the refusal of believing the stressor is real and can useful by minimizing the distress or alternatively harmful by creating more problems through ignoring the initial stressor.11 Acceptance involves taking the reality of the situation as is and attempting to deal with it.11 Religious coping is the act of turning to religion as emotional support or positive growth.11 Substance use is defined as using drugs and/or alcohol or other substances to reduce stress and is considered a destructive coping skill.12, 13 Finally, humor is described as making light of a problem or diverting its negative attention.10, 12, 13
Psychosocial interventions (i.e. active coping) have been proven to reduce symptoms of stress and increase functioning, but unfortunately these healthy coping skills are not often used.8 The lack of problem-focused coping skills can lead to further psychological and physiological deterioration.1,8 Additionally, if improperly managed, stress can lead to, but is not limited to burnout, anxiety, depression, personal and professional difficulties, and suicidal ideations.8 Depression, for example, is common in those who lack constructive, problem-focused coping skills.14 This occurs more commonly in medical students compared to the general population.14
With the information presented, researchers sought to determine the level of perceived stress experienced, the types of coping skills medical students use to mitigate stress, and what affect PS and the 15 coping skills have on biological sex, year in school, and age. Researchers hypothesized females, younger students, and those in the earlier years in medical school to have greater levels of PS, compared to other sexes, older students, and the later years of medical school, respectively. Additionally, based on previous research and theory, researchers hypothesized medical students to have greater use of emotion-focused coping skills. Finally, researchers hypothesized greater use of emotion-focused coping skills in females, younger students, and those in earlier years of medical school.
METHODS
Setting and Participants
This research was executed at a college of osteopathic medicine (COM). Participants consisted of medical students in years one through four; all other programs were excluded from this study. Participants were recruited via an institutional email. Participation was voluntary. An institutional review board approved this research (CHS-18-7-CHS) and informed consent was gathered electronically. STROBE guidelines were used to guide this research and writing.
Instrumentation
A survey was used to gather data; it was distributed via email. Surveys were administered via Qualtrics (Qualtrics Inc., Provo, UT). The first portion of the survey included a researcher-produced measure of demographics: age, biological sex, and year in the COM. The second portion involved two different instruments to measure stress and coping. To measure stress, researchers chose the Perceived Stress Scale (PSS).15 For coping, the Coping Orientation to Problem Experience inventory (COPE) was chosen.11
Perceived Stress Scale
The Perceived Stress Scale (PSS) is a 10 question self-report instrument intended for measuring perception of general stress within the past month.15 Items are rated on a 5-point Likert scale ranging from “never” to “very often.” The instrument has a Cronbach’s alpha of α=0.78 for reliability.15 Additionally, a sixth response “prefer not to respond” was added for further discretion. Scoring involved tallying responses to questions 1, 2, 3, 6, 9, 10 (negatively stated items) and reverse scoring for responses to questions 4, 5, 7, 8 (positively stated items).15 Questions marked as “prefer not to answer” were recorded as zero. Scores 0-13 indicate lower stress, 14-26 moderate, and 27-40 as high perceived stress.
Coping Orientation to Problem Experience Inventory
The Coping Orientation to Problem Experience inventory (COPE) is a 60 question self-report instrument, divided into 15 different sub-scales described in the next section, and was developed to assess a large range of coping responses.11 The instrument uses a 4-point Likert scale ranging from “I usually don’t do this” to “I usually do this a lot.” Additionally, a fifth response of “prefer not to respond” was included for discretionary purposes and tallied as zero. Larger sums on a specific sub-scale indicate a strong style of coping (maximum of 16).16 The COPE scale has a Cronbach’s alpha of α=0.73 for reliability.10
The COPE contains 15 different sub-scales of coping into which the responses are coded, based on problem-focused or emotion-focused coping.11 Sub-scales include: positive reinterpretation and growth, mental disengagement, focus on and venting of emotions, use of instrumental social support, active coping, denial, religious coping, humor, behavioral disengagement, restraint, use of emotional social support, substance use, acceptance, suppression of competing activities, and planning.11 Carver et al11 explains each of the sub-scales in his theoretical approach in developing the COPE scale. Later research divided the two main styles of coping into four groupings: self-sufficient (problem focus), avoidant, socially supported, and self-sufficient (emotion focus).10 Behavioral and mental disengagement, denial, and substance use are all considered avoidant, or dysfunctional coping mechanisms.10 The remaining 11 demonstrate greater constructive coping.10
Statistical Analysis
Survey data was entered into IBM SPSS 24.0 for analysis. Independent t-tests and Mann-Whitney tests were used to compare biological sex against PS and then again against the 15 coping skills. One-way analysis of variance and Kruskal-Wallis tests were used to determine significance between school year and PS and then again comparing the 15 coping skills; the same was executed for age. Finally, a multiple regression analysis was used to predict the level of PS by the 15 coping skills. Significance was measured at α=0.05.
RESULTS
Sixty-seven COM students completed the survey, with two students omitting their age, (M=27.07, SD=4.49). More males completed the survey (n=37), than females (n=30). Although the option was given for varying biological sex identifiers, males and females were the only biological sexes selected. Each scale (PSS and COPE) was summed separately per participant. School year frequencies are displayed in Table 1.
Table 1: School Year Frequencies
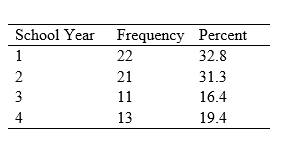
School Year Frequencies
All assumptions were checked before each analysis was conducted. A reliability analysis was executed for each of the scales; PS had an internal reliability with a Cronbach’s alpha of α=0.80, and Cronbach’s alpha for COPE of α=0.65.
Medical Student Stress Level
Perceived Stress for COM students was reported as M=15.91, (SD=7.60), or “moderate” PS. An independent t-test revealed significance for PS with biological sex (N=67), 30 females had a greater level of PS (M=18.50, SD=7.28), than 37 males (M=13.81, SD=7.29), t(65)=2.62, p=0.01. No significance was observed with younger students (F(19,45)=1.21, p=0.30) and those in the early years of medical school (F(3,63)=0.31, p=0.82).
Predicting Level of Perceived Stress through Type of Coping Skill Use
The goal of determining the ability of each of the coping skills to predict level of PS was explored by performing a standard multiple regression. Preliminary analyses were performed to ensure there was no violation of the assumption of normality and linearity. Outliers were previously removed for the ANOVAs and t-tests. Social support and emotional support both demonstrated high multicollinearity. Because social support did not demonstrate statistical significance, it was removed as a predictor variable. With its removal, no predictors demonstrated multicollinearity. Upon full interpretation of the regression, the linear combination of the 14 coping skills (positive reinterpretation and growth, mental disengagement, focus on and venting of emotions, active coping, denial, religious coping, humor, behavioral disengagement, restraint, use of emotional social support, substance use, acceptance, suppression of competing activities, and planning) accounted for 64% of the variance in perceived stress, R2=0.71, adjusted R2=0.64. The model demonstrated statistical significance, F(14,52) =9.23, p<0.00. A one unit increase in mental disengagement is associated with a 0.35 increase in PS (β=0.35, t(50)=3.90, p<0.00); and a one unit increase in venting is associated with a 0.56 unit increase in PS, (β=0.56, t(50)=5.27, p<0.00). Comparatively, a one unit increase in emotional support (another emotion-focused coping skill) is associated with a 0.26 decrease in PS, (β= -0.26, t(50)= -2.28, p=0.03). Finally, the only problem-focused coping skill found to be significant was planning. A one unit increase in planning is associated with a 0.34 decrease in PS, (β= -0.34, t(50)= -2.70, p<0.01). Additional results are displayed in Table 2.
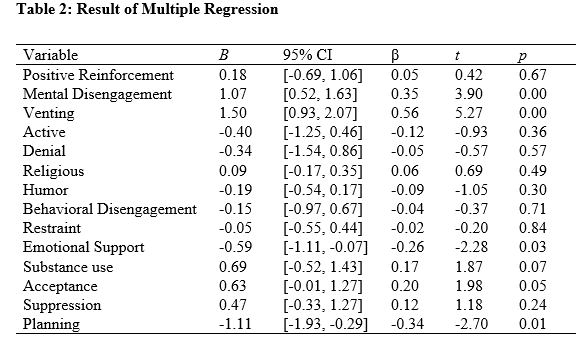
Results of Multiple Regression
Coping Skill Comparisons with Biological Sex, Year in School, and Age
With regard to biological sex, Mann-Whitney tests indicated venting was greater for females (Mdn= 10.00) compared to males (Mdn=7), U(Nfem=30, Nmales=37)=258.00, z= -3.77, p<0.00. Similar results were demonstrated for emotional support, with females (Mdn = 13.50) having greater use than males (Mdn=11.00), U(Nfem=30, Nmales=37)=390.50, z = -2.09, p<0.05. Restraint was the only significant coping skill in which males (M=11.16, SD=2.85) when compared to females (M=9.87, SD=2.21) demonstrated greater use, t(65)= -2.04, p<0.05. Kruskal-Wallis testing demonstrated significance in school year with humor, X2(3)=8.20, p=0.04. Post hoc testing (Games-Howell test) demonstrated significant differences with years 2 and 3, MD= -3.65, p=0.04. Students in their second year were less likely to cope by using humor than those in their third year of medical school. Age did not demonstrate any significance with coping skills.
DISCUSSION
This study aimed to investigate the amount of stress osteopathic medical students perceive to endure and their mechanisms of coping with said stress. Based on the results, it can be inferred that medical students do experience a moderate amount of PS (M =15.91), which aligns with previous research.17, 18 Iorga et al. demonstrated PS M = 17.31 in medical students using the same instrument utilized in this study.17 Additionally, Jabeen et al. discovered similar results with a different version of the PSS, in that medical students experience a moderate amount of PS.18 This level of PS is of concern with medical school experience as it has been associated with increases in depression.17 Additionally, increased stress and depression can negatively influence academic achievement, which can impact error rates with academic and clinic work and can potentially lead to suicidal ideation. It is important to note that when compared to peers in other graduate programs, medical students have higher rates of depression.17,18 The use of avoidant coping skills, such as mental disengagement, may be related to this, as our results demonstrate that it can cause an increase in PS. There is also evidence that stress is cyclical; it can lead to poor academics, which can therefore lead to more stress.19 Furthermore, the increased levels of stress during medical school can have an effect in later life on career and patient care.18 Although the results were as expected, more research is necessary in order to investigate what specific facets of medical school may relate to increases in stress.
Biological Sex and Perceived Stress
Our initial prediction of females reporting higher levels of PS demonstrated statistical significance with females exhibiting higher levels of PS than males. These results are consistent with previous research on medical students and PS.17, 18, 20 According to the American Psychological Association4 females, in general, are more likely to report greater stress than males. However, why this occurs with females and stress still remains unclear.21 Previous research suggests threatening event appraisal, greater exposure of daily stressors, gender roles, relational emotional involvement, psychological development, and endocrinology may all play a role in why females demonstrate higher stress levels, however a definitive cause is unknown.21 Further experimental research on biological sex physiological and psychological processes may assist in the understanding of stress and biological sex differences.
Coping’s Effect on Perceived Stress
The multiple regression results were synonymous with our initial hypothesis of greater use of emotion-focused coping skills in relation to PS. This prediction is also consistent with previous research.19, 22 Three out of four significant predictors were emotion-focused coping skills: mental disengagement, venting, and emotional support. This could suggest that COM students are enduring their stress rather than actively mitigating their stressor.10, 11 Though these three are emotion-focused coping strategies, stress is not mitigated in the same way for all. For example, mental disengagement and venting predicted increases in PS, but emotional support predicted decreases in PS. Previous research has suggested that greater increases in emotion-focused coping can lead to greater increases in stress, which has positive associations with depression.22 Additionally, emotion-focused coping has been associated with decreased academics, especially clinical experience performance and therefore may become detrimental to achievement.19 But why does PS decrease with use of emotional support? Litman’s10 principal components analysis (PCA) of Carver’s11 coping styles may give us a greater explanation.
Emotion-Focused Coping Outcomes
Litman completed a principal components analysis on Carver et al. original 15 subscales that formed the four factors to which the coping skills of each factor demonstrated similar characteristics: self-sufficient problem and emotion focused, avoidant-coping, and socially supported.10,11 Mental and behavioral disengagement, substance, use, and denial are all avoidant-coping, in which the individual will avoid the problem or associated emotions and are considered destructive or detrimental.10, 11 Previous research has indicated that those who use avoidant coping skills, may have lower-self efficacy.23 Self-efficacy is linked to individual’s drive to succeed, dealing with adversity, and ability to cope with challenges.24 When self-efficacy is lacking, it can be a major detriment to academics because of the lack of control over certain situations.23 Venting and emotional support (as well as social support, problem-focus) are “socially-supported,” which have a more socially positive focus. It is suggested that this factor loading is associated with motivation to approach the problem, but fear of negative consequences.10 This concept of fear of consequences more closely aligns with venting. Although it is considered “socially-supported,” venting can be considered negative due to its focus on the stressor, and therefore can become cyclical.10 Litman10 conducted an additional PCA model with three factor loadings and found positive-sloped correlations between venting and anxiety. It may be observed from our introduction that stress and anxiety often occur simultaneously and this could be why an increase of PS in this study is observed with venting. 8,14 Finally, in Litman’s10 three factor model, emotional support demonstrated positive-sloped correlations with positive (beneficial) traits from the Values in Action Inventory of Strength.25 It includes the traits: social intelligence, prudence, hope, humor, spirituality, and perspective.25 A negative-sloped correlation with anxiety.10 This also aligns with the results of this study.
Problem-Focused Coping Outcomes
The results of this study demonstrated a decrease in PS with use of the problem-focused coping skill, planning. Litman’s10 three and four factor PCA models placed planning in the self-sufficient, problem-focused factor.11 The self-sufficient coping factors are related to approach-based motives, positive traits in the Values in Action Inventory of Strength, and have demonstrated negative relationships with avoidant coping strategies.10, 25 The results also aligned itself with previous research which has demonstrated that problem-focused or active strategies will more likely have an improved outcome when modifying stressful situations than emotion-focused coping.22 Finally, in terms of medical school, the use of self-sufficient (problem-focused) coping mechanisms has been associated with improved clinical performance.19
Biological Sex and Coping
When comparing biological sex and coping skills, venting and emotional support demonstrated significance with females, while restraint was significant in males. Previous research demonstrates that males use their social networks to normalize emotional stress and bring it under control by “forgetting about it”, while females use their social networks more so for awareness of emotional distress or “talking about it.”26 This is relational to this study, at least for females, in their use of emotion-focused coping and venting. Males demonstrated significance with restraint in the study. Restraint, the act of waiting for the right moment to approach a stressor, is a problem-focused coping skill which has shown to have greater effects on mitigating stress due to its confrontational use.19 When exploring more into the male “forgetting about it” approach, it is suggested that this type of coping helps them maintain a level of self-control, which may be a form of a restraint.26 Finally, an abundance of research suggest that males are more likely to use problem-focused coping strategies, while females use emotion-focused.26, 27, 28, 29, 30 This use of emotion-focused coping has suggested greater psychological distress in females, as well as greater reports of depression and anxiety.29, 30
School Year and Humor
The last significant result demonstrated that third-year medical students are more likely to use humor as a coping skill than second-year students. Typically, in the third year, students transition from didactic learning to clinical learning, involving direct patient interaction and care.31 Previous research suggests that the third year may be the most challenging time for medical students, due to exposure to multiple stressful and potentially traumatic events (such as patient suffering, death, personal mistreatment, and poor role-modeling by physicians).31, 32, 33 These outcomes can cause an increase in anxiety and depression.31 However, this trauma has not been associated with poor outcomes by the end of the third year, suggesting resilience with these students.31 This resilience has been related to support from others, especially their own team members.31 Links between resilience and humor have been studied in prisoners of war who have experienced post-traumatic stress, suggesting that humor and resilience are both elements of communication and connection.34 This construct of human connection and communication has contributed to survival and resilience, with the implication that resilience is contagious, just as humor appears to be.34 Humor and resilience allowed these prisoners of war to draw elements of mastery and independence from each other, allowing for greater coping.34 Though war is not comparable to medical school, the trauma caused from each may be similar and this is why a connection is suggested between trauma and humor.
Limitations
Although many significant pieces of information were discovered through this study, it is not without limitation. First, the sample of this study includes students from one university and may lack generalizability. More diversity in results might have been observed if more programs were included. Secondly, the sample size was smaller than expected. A larger sample may have yielded more robust results. The survey involved over 60 items which may have created survey-fatigue and discouraged participants from completing it. Finally, this research occurred before the COVID-19 Pandemic, which significantly altered life as we know it.
Conclusion
In summary, the results of this study research suggest that medical students experience a moderate amount of stress, specifically females. The students mostly use emotion-focused coping strategies to mitigate stress, which have shown increased stress rather than decreased. Finally, third-year students have greater use of humor, as it is part of resilience and communication. This research is noteworthy for medical school faculty, administrators, and students when considering medical school and the underlying factors that accompany it. One should consider their mental health before pursuing application to medical school. Future research should explore avenues to mitigate these stressors, and shift to constructive coping methods to improve overall academic and clinical performance in medical school, clinical work, residency, and as a professional.
References
1. Van Burkel K, Reeves B. Stress among graduate students in relation to health behaviors. Coll Stud J 2017;51(4):498-510.
2. Lovallo WR. Stress & Health Biological and psychological interactions. Thousand Oaks, California: Sage Publications Inc; 2005.
3. Gallop Inc. Gallup Global Emotions. 2019. https://www.gallup.com/analytics/248909/gallup-2019-global-emotions-report-pdf.aspx. Accessed 15 September 2019.
4. APA, American Psychological Association. Stress in America: Stress and sex. 2010. https://www.apa.org/news/press/releases/stress/2010/sex-stress.pdf. Accessed 10 January 2020.
5. Darabi M, Macaskill A, Reidy L. Stress among UK academics: identifying who copes best. J Further High Educ. 2017;41(3):393-412.
6. Dyrbe LN, West CP, Satele D, Boone S, Tan L, Sloan J, Shanafelt TD. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451.
7. Kotter T, Tautphaus Y, Obst KU, Voltmer E, Scherer M. Health-promotion factors in freshman year of medical school: A longitudinal study. Med Educ. 2016;50(6):646-656.
8. Hassan El-Ghoroury N, Galper DI, Sawaqdeh A, Bufka LF. Stress, coping, and barriers to wellness among psychology graduate students. Train Educ Prof Psychol. 2012;6(2):122-134.
9. Lazarus RS, Folkman S. Transactional theory and research on emotions and coping. Eur J Pers. 1987;(3):141-169
10. Litman J. The COPE inventory: Dimensionality and relationships with approach- and avoidance-motives and positive and negative traits. Pers Individ Dif. 2006;41:273-284.
11. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. Pers Soc Psychol Rev. 1989;56:267-283.
12. Carver CS, Scheier MF. A control-theory model of normal behavior, and implications for problems in self-management. Adv Cogn-Behav Res Ther. 1983;2:127-194
13. Hull JG. A self-awareness model of the causes and consequences of alcohol consumption. J Abnorm Psychol. 1981;90:518-530.
14. Dagistani A, Al Hejaili F, Binsalih S, Al Jahdali H, Al Sayyari A. Stress in medical students in a problem-based learning curriculum. Int J High Educ. 2016;5(3):12-19.
15. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385-396
16. Cook SW, Heppner PP. A psychometric study of three coping measures. Educ Psychol Meas. 1997;57(6):906-923.
17. Iorga M, Dondas C, Zugun-Eloae C. Depressed as freshmen, stress as seniors: the relationship between depression, perceived stress and academic results among medical students. Behav Sci. 2018;8(70):1-12.
18. Jabeen A, Iqubal S, Sheikh GM, Riaz F. Comparison of perceived stress and sources of stress in students of basic, preclinical and clinical levels of medical education. ISRA Med J. 2019; 11(1):51-54.
19. Schiller JH, Stansfield RB, Belmonte DC, Purkiss JA, Reddy RM, House JB, Santen SA. Medical students’ use of different coping strategies and relationship with academic performance in preclinical and clinical years. Teach Learn Med. 2017;30(1):15-21.
20. Reddy EA, Raju Srijampana VV, Rajana B, Muddana ST. Perceived stress and prevalence of depression among first-year medical students. J NTR Uni of Health Sci. 2015; 4:209-213.
21. Pilar Matud M. Sex differences in stress and coping skills. Pers Individ Dif. 2004; 37:1401-1415.
22. Mosley Jr. TH, Perrin SG, Neral SM, Dubbert PM, Grothues CA, Pinto BM. Stress, coping, and well-being among third-year medical students. Acad Med. 1994; 69(9):765–7.
23. Thomasson P, Psouni E. Social anxiety and related social impairment are linked to self-efficacy and dysfunctional coping. Scand J Psychol. 2010;51:171-178.
24. Chemers MM, Hu L, Garcia BF. Academic self-efficacy and first-year college student performance and adjustment. J Educ Psychol. 2001;93:55-64.
25. Peterson C, Seligman MEP. Character strengths and virtues: a handbook classification. Oxford Uni Press. 2004.
26. Martinez-Hernaez A, Carceller-Maicas N, DiGiacomo SM, Ariste S. Social support and sex differences in coping with depression among emerging adults: a mixed-methods study. Child and Adolesc Psychiatry and Ment Health. 2016; 10(2).
27. Endler NS, Parker JDA. Multidimensional assessment of coping: A theoretical analysis. J Pers Soc Psychol. 1990;58:844–854.
28. Matud MP. Sex differences in stress and coping styles. Pers Individual Differ. 2004;37:1401–1415.
29. Ptacek JT, Smith RE, Dodge KL. Sex differences in coping with stress: When stressors and appraisal do not differ. Pers Soc Psychol Bull. 1994;20:421–430.
30. Mazure CM, Maciejewski PK. The interplay of stress, sex and cognitive style in depressive onset. Arch Womens Ment Health. 2003;6:5–8.
31. Haglund MEM, Rot MAH, Cooper NS, Nestadt PS, Muller D, Southwick SM, Charney DS. Resilience in the third year of medical school: A prospective study of the associations between stressful events occurring during clinical rotations and student well-being. Acad Med. 2009; 84(2): 258-268.
32. Radcliffe C, Lester H. Perceived stress during undergraduate medical training: A qualitative study. Med Educ. 2003;37:32–38. 8
33. Rosenthal JM, Okie S. White coat, mood indigo—Depression in medical school. N Engl J Med. 2005;353:1085–1088.
34. Henman LD. Humor as a coping mechanism: Lessons from POWs. Humor. 2008; 83-94.