Perception of Pain with IUD Insertion in Nulliparous Women vs Multiparous Women: A Systematic Review
Emily DuBuc, B.S., Office of Medical Student Research, Oklahoma State University Center for Health Sciences, Tulsa, Oklahoma
Kimberly Magana, M.Ed., Office of Medical Student Research, Oklahoma State University Center for Health Sciences, Tulsa, Oklahoma
Micaela Motzko, D.O, Department of Obstetrics and Gynecology, Oklahoma State University Medical Center, Tulsa, Oklahoma
Lauren Thomas, D.O, Department of Obstetrics and Gynecology, Oklahoma State University Medical Center, Tulsa, Oklahoma
Corresponding Author: Ms. Emily DuBuc, Oklahoma State University Center for Health Sciences, Address: 1111 W 17th St., Tulsa, OK 74107, United States, Email: emily.dubuc@okstate.edu, Phone: 918-582-1972
Contact Information for authors:
Emily DuBuc - emily.dubuc@okstate.edu
Kimberly Magana - kimberly.magana@okstate.edu
Micaela Motzko - mmotzko@okstate.edu
Lauren Thomas - Lauren.chinnery@okstate.edu
Statement of Authorship: As corresponding author, I confirm that the manuscript has been read and approved for submission by all the named authors.
Funding: None
Conflicts of Interest: No financial or other sources of support were provided during the development of this manuscript.
Acknowledgements: None
Duplicate publication statement: the authors above have not published or submitted any related papers from the same study.
Abstract:
Importance: Intrauterine devices (IUD) are a popular form of long-acting reversible contraception that are highly effective. However, a common hesitation to abstain from this form of contraction is the perceived pain during the insertion procedure. Recognizing and addressing this common perception will help obstetricians and gynecologists guide care for their patients. This study aims to perform a review of published literature to quantify the pain experienced during insertion for nulliparous women compared to multiparous women.
Methods: A search string focused on IUDs developed by a systematic review librarian was applied to Embase and PubMed. Returns were uploaded to Rayyan, a systematic review screening platform. In a masked, duplicate fashion, authors (E.D., K.M.) independently screened the titles and abstracts to determine inclusion in this analysis. Data was extracted in a masked, duplicated fashion, using a pilot-tested Google form. Results are reported with both frequencies and percentages to determine the presence of any relationships.
Findings: Twenty-eight studies analyzed both parous and nulliparous women of which 14 studies directly stated that IUD insertion is more painful in nulliparous women (14/28, 50%). 28 studies analyzed both parous and nulliparous patients (28/49, 57.1%), 18 analyzed nulliparous patients only (18/49, 36.7%). The most common pain measurement tool used was a Visual Analogue Scale (VAS) (41/49, 83.7%). Pain interventions were used in 36 studies (36/49, 73.5%).
Conclusions and Relevance: After review, we found that there is limited research measuring patient pain during IUD insertion. Based on the included studies, pain intervention should be a discussion between the provider and the patient to determine the best course of action. There is a need for further research on this topic in an effort to update current protocols regarding pain intervention.
Introduction:
Intrauterine devices (IUD) are a popular form of long-acting reversible contraception (LARC) that are highly effective.1 It is estimated that in the United States between 2017-2019, 10.4% of women between the ages of fifteen and forty-nine used an IUD or contraceptive implant as their main form of contraceptive 1. This number has only increased since the IUD has gained popularity. However, a common barrier to IUD access is the perceived pain during the insertion. Review of the most liked videos related to #IUD on TikTok, a video-sharing social media app, shows that when patients share their personal experience with IUDs, 80.6% will have a negative tone and 25% will emphasize the desire for anesthesia during placement 2. In a cohort study done by Santos et al, almost all women surveyed reported some degree of pain at insertion, regardless of parity, form of delivery, or IUD type3. The insertion is offered as an in-office procedure with varying use of pain interventions, with some gynecologists opting to forego pain interventions completely due to the short duration of the procedure. Studies have been conducted to compare the different pain intervention methods such as verbal anesthesia, Naproxen, Misoprostol, and Lidocaine with no concise recommendation on which is superior 4. In a systematic review of literature performed by Gemzell-Danielsson et al., there was no conclusive evidence that any prophylactic pharmacological intervention reduces pain associated with IUD insertion.5 It has been proposed that the ease of the insertion depends on factors such as the dilation of the cervix, ease of locating the cervix, and skill level of the provider. It has also been proposed that pain during insertion is highly dependent on parity, with the procedure being more painful in nulliparous women 6. This is because the cervix has not been previously dilated and therefore might require mechanical or pharmacologic methods to allow for insertion.7 The process of dilation itself can also contribute to the pain patients experience. Parous women maintain a slight cervical dilation after vaginal childbirth that may make the IUD insertion easier and less painful7. Common complications that can arise during cervical dilation for insertion include bleeding, vasovagal-like reactions due to pain, and uterine perforation.8
Despite the growing interest in IUDs, there is still limited evidence to quantify pain during this procedure. We conducted a review of published literature to analyze the relationship of perceived pain during an IUD insertion by nulliparous and multiparous women. We also reviewed treatment measures that were received by these patients and the effects they had on the reported pain scale. Our primary goal is to perform a review of published literature to quantify the pain experienced during insertion for nulliparous women compared to multiparous women.
Sources/ Study selection Methods:
In this literature review, using PubMed and Embase, a systematic review librarian at Oklahoma State University - Center for Health Sciences identified publications using the following keywords: “nulliparous,” “parity,” “gravida,” cross-referencing with “IUD or intrauterine device” and “insert” and “pain” from January 1, 2013 to March 1, 2024. After the searches were conducted, the returns were uploaded to Rayyan, a systematic review (SR) screening platform. Eligibility criteria included any study in which there was an evaluation of pain during the IUD insertion. We also accepted any study in which ease of the procedure was documented and described how the patient tolerated IUD insertion, as reported by the patients themselves. We
excluded studies that included participants under the age of 15 or did not record the pain during the procedure. We included the following study designs: systematic reviews, retrospective database reviews, cross-sectional analysis, and cohort studies. We excluded retracted articles, commentaries, correspondences, and letters to journals due to their inconsistency in reporting original research. Additionally, we excluded any study unrelated to IUD insertion and any study written in a language other than English. All abstracts were screened and, if they met the inclusion criteria, the full text was reviewed before being included in our literature review. Abstract screening and full text review was done in a masked, duplicate fashion by two investigators (ED, KM), and the manuscripts were then either included or rejected based on the criteria. If there was any discrepancy, the abstract was sent to the physician investigator for further review. The protocol, search string, raw data, and extraction forms were uploaded to Open Science Framework. We conducted this literature review of the perception of pain with IUD insertion in nulliparous and multiparous women according to the Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) guidelines. Fifty-one articles met criteria and were eligible for data extraction. Two authors (ED, KM) used a pilot-tested Google form to extract data from included publications. General characteristics extracted from each study were the PubMed ID or DOI, year study was received (or published if the received date was not available), author names, and conflict of interest statement. Investigators also extracted if pain was evaluated, the measures used to rate pain, if the patient population was nulliparous or parous, interventions used to decrease pain, and patients’ rating of pain experienced during insertion. This manuscript was granted an exemption from the Oklahoma State University – Center for Health Sciences IRB.
Results:
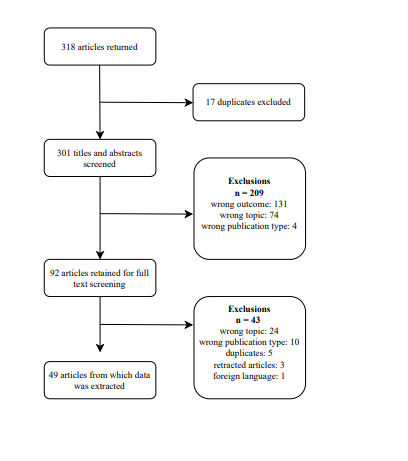
Our literature search yielded 318 returns, of which 17 were duplicates and removed. The title and abstracts were screened and an additional 210 were excluded. Ninety-two articles were retained for full text review, of which 43 were excluded (Figure 1). Our final sample included 49 articles. The most common study design in our sample was randomized controlled clinical trials (33/49, 67.3%) followed by cohort studies (5/49, 10.2%) and systematic reviews (4/49, 8.2%). Regarding parity, 28 studies analyzed both parous and nulliparous patients (28/49, 57.1%), 18 analyzed nulliparous patients only (18/49, 36.7%) and 3 analyzed parous patients only (3/49, 6.1%). The most common pain measurement tool used was a Visual Analogue Scale (VAS) (41/49, 83.7%). Pain interventions were used in 36 studies (36/49, 73.5%). Of the 36 studies evaluating pain interventions, 3 looked at parous only (3/36, 8.3%), 16 looked at nulliparous only (16/36, 44.4%), and 17 looked at both parous and nulliparous (17/36, 42.2%). The most common pain intervention studied was misoprostol (10/36, 27.8%), followed by a lidocaine block (8/36, 22.2%) and lidocaine gel (8/36, 22.2%). Twenty-eight studies analyzed both parous and nulliparous women, of which 14 studies directly stated that IUD insertion is more painful in nulliparous women (14/28, 50%).
Discussion:
Our findings revealed that there are only 49 studies that analyze pain during the insertion of an IUD in parous versus nulliparous women. This is not enough research to make a definitive claim on the average pain scale rating for parous women vs nulliparous women. The lack of research into this topic could be attributed to providers not recognizing pain as a barrier to care or the dismissal of pain due to the short nature of the procedure. With the average time of the procedure being around 555 seconds or 9.25 minutes in young adults, the providers could see this as a reason not to prescribe pain interventions 9. There are also not enough studies that compare all possible pain intervention methods to create a data-supported recommendation on which is the most effective in reducing pain. In our analysis, misoprostol was the most studied pain intervention. Misoprostol is a prostaglandin E1 and works to dilate and soften the cervix prior to the procedure 10. There is an argument of whether or not it can be considered a “pain intervention” as it causes cramping and discomfort as it works to dilate the cervix. This dilation, especially for nulliparous women, allows for an easier insertion for providers, which shortens the procedure and may overall decrease experienced pain. Out of the studies that compared pain in
parous vs nulliparous women, the majority showed that IUD insertion is more painful in nulliparous women. This could be because a nulliparous cervix is closed and has never been dilated to the degree of a parous cervix. In fact, a parous cervix does not fully return to a closed position, and this slight dilation makes IUD insertion easier. 6 The strengths of this study include screening and data extraction were done in a masked duplicate fashion to limit bias, and articles were reviewed and analyzed in a standardized procedure. Limitations of this study include the limited availability of data and the lack of a mandated approach for studies to evaluate the pain during insertion. Most studies use the visual analogue scale, but others used patient reported descriptors of pain such as “mild,” “moderate,” or “severe,” depending on what that word means to the participant. Without a mandated approach, it is difficult to calculate a precise number and compare the perceived pain between different studies. However, the data we collected does suggest that this procedure is associated with a varying amount of pain and the option of utilizing pain medication should be discussed with the patient prior to the procedure. There is a need for more research on this topic to update current protocols regarding pain intervention.
References
1. Daniels K, Abma JC. Current contraceptive status among women aged 15–49: United States, 2017–2019. NCHS Data Brief, no 388. Hyattsville, MD: National Center for Health Statistics. 2020.
2. Wu J, Trahair E, Happ M, Swartz J. TikTok, #IUD, and User Experience With Intrauterine Devices Reported on Social Media. Obstet Gynecol. 2023 Jan 1;141(1):215-217. doi: 10.1097/AOG.0000000000005027. Epub 2022 Dec 5. PMID: 36473194; PMCID: PMC9892286.
3. Santos AR, Bahamondes MV, Hidalgo MM, Atti A, Bahamondes L, Monteiro I. Pain at insertion of the levonorgestrel-releasing intrauterine system in nulligravida and parous women with and without cesarean section. Contraception. 2013 Jul;88(1):164-8. doi: 10.1016/j.contraception.2012.10.015. Epub 2013 Mar 15. PMID: 23507169.
4. Nguyen L, Lamarche L, Lennox R, Ramdyal A, Patel T, Black M, Mangin D. Strategies to Mitigate Anxiety and Pain in Intrauterine Device Insertion: A Systematic Review. J Obstet Gynaecol Can. 2020 Sep;42(9):1138-1146.e2. doi: 10.1016/j.jogc.2019.09.014. Epub 2019 Dec 25. PMID: 31882291.
5. Gemzell-Danielsson K, Apter D, Lukkari-Lax E, Roth K, Serrani M. Overcoming barriers to levonorgestrel-releasing intrauterine system placement: an evaluation of placement of LNG-IUS 8 using the modified EvoInserter® in a majority nulliparous population. Contraception. 2017 Dec;96(6):426-431. doi: 10.1016/j.contraception.2017.08.004. Epub 2017 Aug 24. PMID: 28844878.
6. Branger B, Priou E, David P. Dispositif intra-utérin au cuivre (DIUc) : comparaison de la tolérance et de l’efficacité chez des nullipares et des multipares sur 6 mois [Copper-
containing intrauterine device (cIUD): Comparison of tolerance and efficacy in nulliparous and parous women over 6 months]. Gynecol Obstet Fertil Senol. 2021 Dec;49(12):897-906. French. doi: 10.1016/j.gofs.2021.06.004. Epub 2021 Jun 16. PMID: 34144222.
7. Barone WR, Feola AJ, Moalli PA, Abramowitch SD. THE EFFECT OF PREGNANCY AND POSTPARTUM RECOVERY ON THE VISCOELASTIC BEHAVIOR OF THE RAT CERVIX. J Mech Med Biol. 2012 Mar;12(1):12500091-125000917. doi: 10.1142/S0219519412004399. PMID: 23125473; PMCID: PMC3487462.
8. de Oliveira ECF, Baêta T, Brant APC, Silva-Filho A, Rocha ALL. Use of naproxen versus intracervical block for pain control during the 52-mg levonorgestrel-releasing intrauterine system insertion in young women: a multivariate analysis of a randomized controlled trial. BMC Womens Health. 2021 Oct 29;21(1):377. doi: 10.1186/s12905-021-01521-z. PMID: 34715839; PMCID: PMC8556879.
9. O'Flynn, O'Brien KL, Akers AY, Perriera LK, Schreiber CA, Garcia-Espana JF, Sonalkar S. Intrauterine Device Insertion Procedure Duration in Adolescent and Young Adult Women. J Pediatr Adolesc Gynecol. 2019 Jun;32(3):312-315. doi: 10.1016/j.jpag.2019.01.002. Epub 2019 Jan 8. PMID: 30633980; PMCID: PMC6570557.
10. Goldberg AB, Carusi DA, Meckstroth KR. Misoprostol in gynecology. Curr Womens Health Rep. 2003 Dec;3(6):475-83. PMID: 14613669.