Shannon Headley, D.O., Oklahoma State University Center for Health Sciences, Department of Pediatrics Tribal-Rural Track, Tahlequah, Oklahoma
Blakelee Eggleston, BPH, Oklahoma State University College of Osteopathic Medicine at Cherokee Nation, Office of Medical Student Research, Tahlequah, Oklahoma
Amy Hendrix-Dicken, M.A., University of Oklahoma School of Community Medicine, Department of Pediatrics, Tulsa, Oklahoma
Laura Campion, M.D., University of Oklahoma School of Community Medicine, Department of Pediatrics, Tulsa, Oklahoma
Micah Hartwell, Ph.D. Oklahoma State University College of Osteopathic Medicine at Cherokee Nation, Office of Medical Student Research, Tahlequah, Oklahoma Oklahoma State University Center for Health Sciences, Department of Psychiatry and Behavioral Sciences, Tulsa, Oklahoma
Corresponding Author: Molly Bloom, Oklahoma State University Center for Health Sciences Address: 1111 W 17th St., Tulsa, OK 74107, United States. Email: molly.bloom@okstate.edu Phone: (580) 402-5266
Ethical Statement: This study was determined to be non-human subjects research by the Oklahoma State University Institutional Review Board. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Conflicts of interest/Declarations: Dr. Hartwell receives research funding from the National Institute of Child Health and Human Development (U54HD113173; Shreffler), Health Resources and Services Administration (U4AMC44250-01-02, PI: Audra Haney; R41MC45951 PI: Hartwell), and previously from the National Institute of Justice (2020-R2-CX-0014 PI: Beaman)—all unrelated to the current presentation.
Acknowledgments: This research was supported in part by the Health Resources and Services Administration (U4AMC44250-01-02, Audra Haney, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Health Resources Services Administration.
Abstract
Background: Patient-and family-centered care (PFCC) requires partnerships among healthcare professionals, patients, and families. Research shows that PFCC improves health outcomes, enhances patient and family satisfaction, and reduces healthcare costs.
Methods: This study conducted a cross-sectional analysis of the National Survey of Children’s Health (NSCH) 2020-2021 to determine rates of parent-reported PFCC among US children. Researchers utilized NSCH-defined family-centered care and shared decision-making variables, scored from 1 (never) to 4 (always). The study calculated state and national averages, combined them to create a PFCC index, and visualized the data into heat maps.
Results: The study’s PFCC index ranged from 3.45-3.74 with a national average of 3.59 (SD=0.58).
Conclusion: The number of board-certified pediatricians per 100,000 children follows the trend of PFCC rankings, suggesting the need for advocacy for federal funding for medical education. Further, limited English proficiency may hinder PFCC, highlighting the need for guidelines regarding medical interpreters.
Keywords: Pediatrics, Patient and Family-Centered Care, Family-Centered Care, Shared-decision making
Introduction
When searching for outstanding healthcare quality, surveys of patients have identified patient partnership and family inclusion to be among the most sought-after traits.1 The Institute for Patient-and Family-Centered Care defines patient-and family-centered care (PFCC) as an approach to the planning, delivery, and evaluation of healthcare grounded in mutually beneficial partnerships among healthcare professionals, patients, and families.2 The core concepts include dignity and respect, information sharing, participation, and collaboration.2 This approach to care is especially important in pediatric care, and as the American Academy of Pediatrics states, is vital to raising healthy children as it empowers families, promotes cooperation, and creates a comfortable environment for families, parents, and healthcare professionals to discuss any issues.3 PFCC in pediatrics is based upon the understanding that a child’s primary source of strength and support is the family, and their perspectives are important in clinical decision-making.4 Multiple studies have provided evidence that a PFCC approach to care leads to better health outcomes, greater patient and family satisfaction, decreased healthcare costs, and more effective use of healthcare resources. 5–9
One study found that children receiving post-tonsillectomy care recovered faster and were discharged earlier if their mothers were involved in their care.4,5 Additionally, another study found that when parents of infants in the NICU received more PFCC they reported greater satisfaction in the care they received, demonstrated increased competence and confidence in caregiving, and were more willing to seek help from healthcare providers.4,10 Prompted by the accumulation of evidence-based reports of better outcomes correlating with PFCC, many organizations and programs are encouraging and emphasizing the importance of PFCC. Beginning in 1999, the National Institute for Children’s Healthcare Quality launched a program dedicated to improving the quality of healthcare provided to children with a strong focus on family participation by promoting evidence-based PFCC.4 In 2001, the Institute of Medicine released a report entitled “A New Health System for the 21st Century,” specifying six domains for improvement of healthcare delivery, one of which is patient-centeredness.4 Furthermore, the National Patient Safety Foundation has prioritized the redesign of healthcare systems and processes to promote PFCC in an effort to improve patient safety practices.4
Given the impact of PFCC on patient outcomes and satisfaction, in addition to the numerous programs and organizations aimed towards increasing treatment with PFCC, further evaluation of the implementation is warranted. With a better understanding of where PFCC is the most and least successful, shortcomings and barriers to receiving PFCC treatment can be more readily identified. Through recognition of these barriers, strategies may be proposed to increase PFCC thereby increasing the quality of care and improving patient outcomes for the U.S. pediatric population. Therefore, this study's primary objective was to determine which states had the highest and lowest rates of parent-reported PFCC using data from the National Survey of Children’s Health (NSCH).
Methods
To assess the rates of PFCC in the United States by state, the researchers conducted a cross-sectional analysis using data from the NSCH. The NSCH is a nationally representative dataset collecting data annually by randomly sampling households from all fifty states and Washington D.C. In each household, the survey is completed by a primary caregiver of one child aged 0-17 years. The survey is overseen by the US Census Bureau and funded by the Health Resources and Services Administration’s Maternal and Child Bureau (HRSA MCHB). The survey captures multiple features of a child’s life including their personal well-being and social determinants of health such as access to quality healthcare, neighborhood, school, and social context.11 The study used data from the 2020-2021 cycles.
Patient-and Family-Centered Care
To identify parent-reported rates of patient- and family-centered care researchers first used survey questions which the NSCH defined as family-centered care. If the child had received healthcare during the past 12 months, respondents would answer “always; usually; sometimes; never,” to the following family-centered care survey questions:
1. “During the past 12 months, how often did this child's doctor or other healthcare providers spend enough time with this child?”
2. “During the past 12 months, how often did this child's doctor or other health care providers listen carefully to you?”
3. “During the past 12 months, how often did this child's doctors or other healthcare providers show sensitivity to your family's values and customs?”
4. “During the past 12 months, how often did this child's doctor or other healthcare providers provide the specific information you needed concerning this child?”
5. “During the past 12 months, how often did this child's doctor or other health care providers help you feel like a partner in this child's care?”
The study expanded on the NSCH’s definition to additionally include NSCH-shared decision-making survey questions. If the respondent answered “yes” to the survey question, “During the past 12 months, did this child need any decisions to be made regarding their health care, such as whether to get prescriptions, referrals, or procedures,” respondents were directed to answer the following three questions related to shared decision-making with “always; usually; sometimes; never:”
1. “During the past 12 months, how often did this child’s doctors or other health care providers work with you to decide together which health care and treatment choices would be best for this child?”
2. “During the past 12 months, how often did this child's doctors or other health care providers discuss with you the range of options to consider for their health care or treatment?”
3. “During the past 12 months, how often did this child's doctor or other healthcare providers make it easy for you to raise concerns or disagree with recommendations for this child's healthcare?”
State
The NSCH uses sociodemographic factors as screener variables to better categorize responses. The study utilized the State Federal Information Processing System Code to define the State of the child.
Statistical Analysis
Data from the 2020 and 2021 NSCH cycles was combined and the weights criteria were adjusted as described within the methodology report.12 Patient-and family-centered care variables were recorded numerically with 1 being never, 2 being sometimes, 3 being usually, and 4 being always. Using this scale of 1-4 based on survey responses, the means of the two groups of variables (family-centered care and shared decision-making) were calculated by state. Next, the two groups were averaged together to get a final score–our PFCC index. The data was then visualized into heat maps.
Results
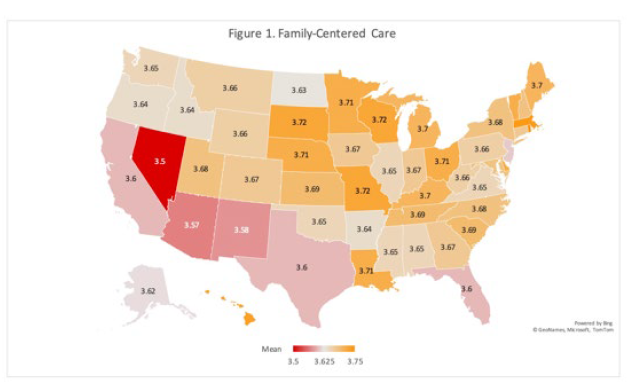
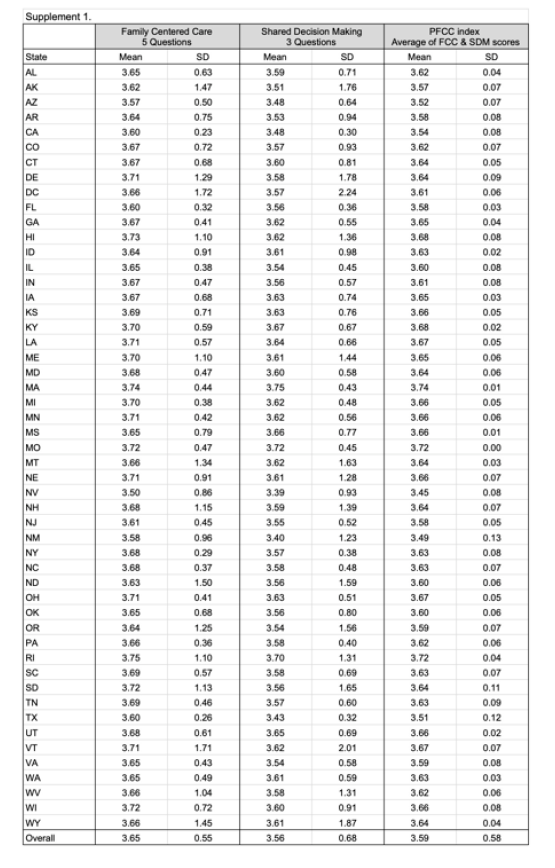
The sample size (n) of our analysis for family-centered care was 77,122 representing a population estimate of 56,815,692 children. Rates of family-centered care in the US ranged from 3.50-3.75 with an overall US average of 3.65 (SD=0.55). Figure 1 shows the rates of family-centered care by state. The top 5 highest ranking states included: Rhode Island (M=3.75, SD=1.10), Massachusetts (M=3.74, SD=0.44), Hawaii (M=3.73, SD=1.10 ), South Dakota (M=3.72, SD=1.13), and Wisconsin (M=3.72, SD=0.72). The lowest 5 ranking states included: Nevada (M=3.50, SD=0.86), Arizona (M=3.57, SD=0.50), New Mexico (M=3.58, SD=0.96), Texas (M=3.60, SD=0.26), and California (M=3.60, SD=0.23).
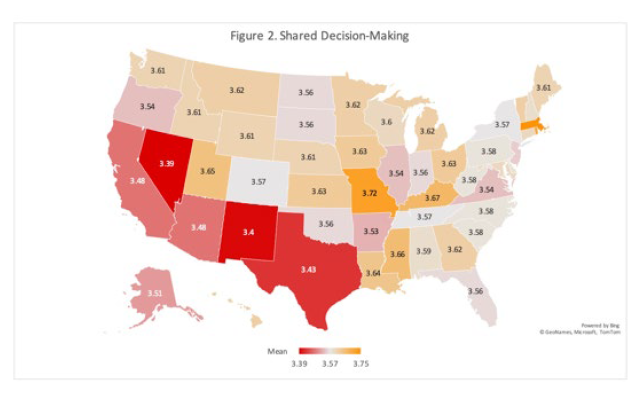
Among the sample size (n=22,294) representing a population of 15,243,434 children, shared decision-making rates in the US ranged from 3.39-3.75 with an overall US average of 3.56 (SD=0.68). Figure 2 shows the rates of shared decision-making by state. The top 5 highest ranking states included: Massachusetts (M=3.75, SD=0.43), Missouri (M=3.72, SD=0.45), Rhode Island (M=3.70, SD=1.31), Kentucky (M=3.67, SD=0.67), and Mississippi (M=3.66, SD=0.77). The lowest 5 ranking states included: Nevada (M=3.39, SD=0.93), New Mexico (M=3.40, SD=1.23), Texas (M=3.43, SD=0.32), Arizona (M=3.48, SD=0.64), and California (M=3.48, SD=0.30).
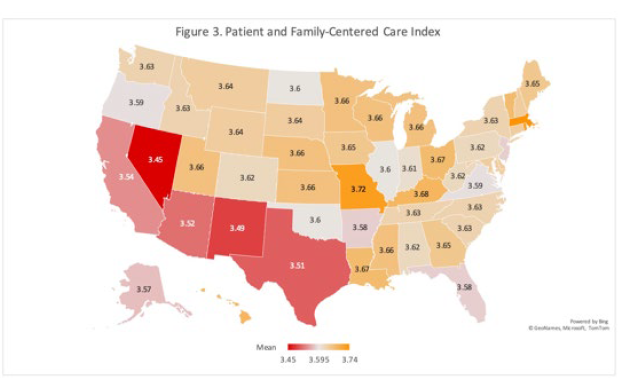
By averaging the family-centered care and shared decision-making rates, the study found the PFCC index to range from 3.45-3.74 with an overall US average of 3.59 (SD=0.58). The sample size (n=22,703) represented a population of 15,100,741 for the study’s adapted definition of PFCC. Figure 3 shows the rates of PFCC by state. The top 5 highest ranking states included: Massachusetts (M=3.74, SD=0.01), Rhode Island (M=3.72, SD=0.04), Missouri (M=3.72, SD=0.002), Kentucky (M=3.68, SD=0.02), and Hawaii (M=3.68, SD=0.08). The lowest 5 ranking states included: Nevada (M=3.45, SD=0.08), New Mexico (M=3.49, SD=0.13), Texas (M=3.51, SD=0.12), Arizona (M=3.52, SD=0.07), and California (M=3.54, SD=0.08).
Discussion
Results from the study showed disparities in PFCC across the United States, with lower ratings found in the Southwestern portion of the US and increasing ratings moving through the Central region and into the Northeast. Massachusetts and Rhode Island were found to have the highest rates of PFCC according to the study, and analysis of CDC data has also found these two states to have the lowest rates of child mortality in the United States. 13 Additionally, excluding Kentucky, the five states with the highest rates of PFCC were found to have higher-than-average child health status, while the opposite is true for the five states with the lowest rates of PFCC.14 This information, when combined with the findings in the study, is suggestive of a relationship between better patient outcomes, including improved morbidity and mortality, and PFCC. Many studies have provided evidence of this relationship, in addition to increasing patient satisfaction and cost savings.4 Considering the impact PFCC has on child health outcomes, identifying barriers to receiving PFCC is crucial.
Given the many influencing and complicated factors related to perceived care delivery performance, there are a variety of system and individual factors that may affect PFCC scores. While the results of this study cannot definitively determine why some states performed better than others, previous research has identified a lack of adequate staffing, physician communication skills, and time as barriers to the level of coordination required for patient-centered care (PCC).15 However, when looking at system-level information that may influence care delivery in underperforming states, one important factor identified within this study is the number of board-certified pediatricians per 100,000 children. According to the American Board of Pediatrics, Nevada is ranked 49th (38.2 per 100k), New Mexico 42nd (54.1 per 100k), Texas 39th (57.6 per 100k), and Arizona 37th (59.2 per 100k).16 This follows the general trends of PFCC rankings across the US—with a notable exception being California (ranked 21st with 75.7 pediatricians per 100k children).16
When comparing the percentage of children in 2021 with an assigned medical home, Nevada (33.2%), New Mexico (39.8%), Texas (42.7%), Arizona (46.9%), and California (42.4%) were all below the national average of 47% which is consistent with the information reported by caregivers in the NSCH.17 It is of interest that the majority of these states' child populations are largely Hispanic, representing between 42%-62% of the population of children ages 0-18.18 While ethnicity alone cannot determine the primary language for families, and certainly cannot account for bilingual medical providers, the large proportion of Hispanic families in bottom-performing states raises concerns that the added complexities of providing care to families with limited English proficiency (LEP) may be hampering the ability of medical teams to provide PFCC. Given that one of the known barriers to PFCC is perceived time, families with LEP may be disproportionately impacted.20 According to the 2019 American Community Survey, the states with the highest percent of their population ages 5+ who spoke a language other than English at home were California (44.5%), Texas (35.6%), New Mexico (34%), New Jersey (32.2%), and Nevada (31.2%) – representing four out of the five states with the lowest PFCC.21 As such, future research should focus on the nativity and primary language of respondents to determine if these factors may influence healthcare experiences for families who have limited English proficiency.
Despite the federal right to language access for individuals with LEP through Title VI of the Civil Rights Act, many healthcare providers are not aware of their responsibility or held accountable through the enforcement of laws.22 Many states have passed additional laws addressing language accessibility in the healthcare setting in an attempt to mitigate this gap in access to care. Interestingly, California–one of the states with the lowest rates of PFCC–has more laws addressing language in the healthcare setting than any other state. 22 However, further investigation reveals considerable flaws in these policies. For example, SB 853: The Health Care Language Assistance Act passed by the California Legislature only provides translated material and language assistance for privately insured individuals.22 As such, this disproportionately affects individuals of lower-income households using public health insurance like Medicare and Medicaid. This is particularly concerning when 32% of 2020’s child enrollee population was Hispanic.23 Furthermore, individuals without health insurance would also be omitted from this law, with non-elderly American Indian and Alaskan Native and Hispanic individuals having the highest rates of uninsured individuals at 21.2% and 19% respectively in 2021.24 This information necessitates the re-evaluation of such laws and policies as they may not be reaching their targeted populations.
Recommendations
In addition to a thorough evaluation of laws and policies in place to essentially promote PFCC, an assessment of state programs designed to increase PFCC is necessary. The patient-centered medical home (PCMH) healthcare delivery model was originally published by the American Academy of Pediatrics in 1967 as an approach to managing the care of children with chronic illnesses.25 Accordingly, it has been associated with effective chronic disease management, increased patient and provider satisfaction, cost savings, improved quality of care, and increased preventative care.26 While 42 states have enacted laws recognizing the PCMH model, only 20 require state health agencies or advisory councils to report to the state legislature on PCMH performances.26 Of those 20, 16 had higher than average PFCC rates according to our study. As this care delivery model has been proven to promote effective disease management and improved patient and provider satisfaction through PFCC, more robust state requirements and enforcement may further promote PFCC.
The Institute of Medicine’s definition of PCC highlights the importance of shared decision-making, and numerous studies have shown that shared decision-making improves patients' satisfaction and involvement with their healthcare.27,28 Massachusetts General, one of the nation’s largest hospitals, was involved in the development of some of the first patient decision aids created in efforts to promote shared decision-making in PCC.29 These patient decision aids come in the form of printed brochures, audio or video presentations, and interactive and web-based materials.30 This, in addition to clinician training on how to use decision aids, has resulted in high rates of PFCC in Massachusetts by helping patients become more involved and informed about their health decision-making.29 A study evaluating primary outcomes based on the International Patient Decision Aid Standards found that the use of decision aids increased participants’ knowledge, accuracy of risk perceptions, and congruency between informed values and care choices compared to usual care.31 Seven states–Maine, Massachusetts, Minnesota, Oregon, Vermont, Washington, and Wisconsin–have begun to promote shared decision-making through the use of these patient decision aids in an attempt to increase PFCC.32 These seven states were all found to have above-average PFCC rates according to this study.
Physician communication, language-concordant care, and cultural awareness
Provider communication skills play a crucial role in achieving patient and family understanding and enabling shared decision-making that aligns with the patient’s goals.33 A majority of currently practicing providers were not taught communication skills via a curriculum with explicit role modeling or techniques and instead learned how to communicate through working experience.33 Several studies have found providers to demonstrate the need for specific training due to the use of medical jargon, blocking patient questions or concerns, and failing to recognize social cues–when the patient is not following or is experiencing emotions from absorbing information.33 The expansion of clinical education and standardized certification courses in communication skills is one way to improve communication skills to provide patients with quality PFCC. One study looking to increase interpersonal communication skills and professionalism evaluated the effectiveness of Crucial ConversationsTM – a standardized two-day program designed to enhance individual skills in high-stakes dialogue.34 They found that implementation of the program significantly improved teamwork climate, safety climate, job satisfaction, stress recognition, perceptions of management, and working conditions.34 Therefore, the utilization of the same or similar programs in medical training or continued education may improve provider communication skills and therefore perceived PFCC.
Although cultural competency is widely accepted in healthcare, many healthcare professionals have difficulty providing culturally competent care.35 While there are policies in place for culturally competent healthcare, there are no clear guidelines or recommendations to ensure providers are knowledgeable or aware of the cultural needs of their diverse patients.35 Employing key strategies at the individual, institutional, and structural levels are all necessary to promote cultural competency and health equity, which contribute to PFCC. These strategies include the production of a diverse workforce with robust professional development and training on interpersonal racism and discrimination, and prioritizing research investigating cultural and racial inequalities and the best practices to mitigate disparities.36 Additionally, working with and designing solutions alongside patients and families with lived experiences and advocating for policy reform to eliminate inequities is needed.36
As previously discussed, access to language-concordant care may also play a significant role in access to PFCC, and many healthcare providers need to be made aware of their responsibility and held accountable for providing this basic need.22 While there are unique complexities to the use of translation services within medical care, research still finds the use of professionally trained medical interpreters to reduce communication errors, improve clinical outcomes, and improve patient satisfaction.37 Development of nationally accepted and enforced guidelines for the training and supply of trained medical interpreters is consequently needed. Further, holding clinic and hospital administration accountable for enforcing these laws, and providing additional time for language access during patient encounters may improve PFCC for individuals with LEP.
Lack of adequate staffing, time, and physician burnout
It is no surprise that inadequate staffing of health care providers may result in poor patient outcomes and quality of care, regardless of the provider’s level of training. One study found that higher staffing levels were associated with reduced medication errors, restraint use, infections, and an overall decrease in the risk of in-hospital mortality by 14%.38 Inadequate staffing is also a likely contributor to poor PFCC as it may decrease the desired amount of time spent with a health care provider while increasing patient wait times, and contributing to provider burnout and compassion fatigue. The Association of American Medical Colleges (AAMC) released a study in 2017 that found the number of new physicians was not keeping pace with the demands of our growing population. 39 Therefore, it is predicted that by 2030 the US will face a shortage of physicians between 40,900 and 104,900.39 Additionally, research shows that due to the COVID-19 pandemic, US hospitals are now experiencing critical staffing shortages.40 For this reason, it is understandable that from 2020 to 2021 there was a significant increase in the amount of physicians experiencing burnout.41 For pediatricians specifically, there was a clinically significant difference in pre- and post-pandemic emotional exhaustion scores with 35% of participants meeting the cutoff for emotional exhaustion pre-pandemic compared to 63% post-pandemic.42 Therefore, the AAMC’s prediction precludes an increase in PFCC in the upcoming years. Furthermore, it anticipates poor patient outcomes and experiences as a result of the cyclical nature of inadequate staffing contributing to time constraints and eventually, provider burnout.
To address the potential barrier of inadequate staffing, and therefore time with patients, the AAMC recommends a complex solution involving delivery innovations, team-based care, and better use of technology.39 The use of telemedicine and virtual visits is one way that healthcare providers have adapted through the COVID-19 pandemic to provide innovative care through the use of technology. Before March 2020, the use of telemedicine in the United States, while on an increasing trajectory, had overall low integration into healthcare due to various restrictions.43 Due to the shelter-in-place orders and COVID-19 surges of infection, Congress made alterations to Medicare restrictions and telemedicine regulations which resulted in a 766% increase in telemedicine encounters throughout the first 3 months of the pandemic.43 Telemedicine and virtual visits have noteworthy feedback from patients, with one study finding 93.2% of individuals reporting that their telemedicine visit was of high quality and 79.0% saying their most recent virtual visit was as thorough as an in-person visit.44 Continued adaptation and further development of telemedicine and virtual healthcare may be necessary to fill the staffing gaps due to provider shortages–particularly in underserved areas. Most importantly, to combat pediatric provider shortages advocating for federal funding for residency positions and expansion of medical school class sizes is necessary to train more physicians, as the AAMC recommends.39
Limitations and Future Research
One significant limitation of this study is that the NSCH relies on parental reporting which is not independently verified and therefore can result in response bias. Additionally, the survey does not include children in foster care or children who are experiencing homelessness. Therefore, the survey may not be an accurate representation of the whole population. Furthermore, the survey answers were obtained during the COVID-19 pandemic, which could produce incomplete or inaccurate results. However, the survey does produce a robust sample size that the authors believe minimizes these limitations. Future research based on this study should include comparing the data obtained in rural versus urban communities as well as assessing the data from a county or zip code level—which are not included in the publicly available NSCH data— to better target specific areas that need improvement.
Conclusion
Patient-and family-centered care is an essential approach to pediatric care and is vital to raising healthy children. Previous research has identified individual factors including lack of adequate staffing, physician communication skills, and time as barriers to receiving PFCC.15 This study identified systemic level factors including the number of board-certified pediatricians per 100,000 children and limited English proficiency to be potential barriers to receiving PFCC. Given these findings, more robust state requirements and enforcement of programs designed to increase PFCC, including the PCMH care delivery model and patient decision aids are needed. Furthermore, advocating for funding, policy change, and further training aimed towards addressing the identified barriers is needed.
References
1. Anderson R, Barbara A, Feldman S. What patients want: A content analysis of key qualities that influence patient satisfaction. J Med Pract Manage. 2007;22(5):255-261.
2. Patient- and Family- Centered Care Defined. Accessed April 23, 2023. https://www.ipfcc.org/bestpractices/sustainable-partnerships/background/pfcc-defined.html
3. Jolley J, Shields L. The evolution of family-centered care. J Pediatr Nurs. 2009;24(2):164-170.
4. COMMITTEE ON HOSPITAL CARE and INSTITUTE FOR PATIENT- AND FAMILY-CENTERED CARE. Patient- and family-centered care and the pediatrician’s role. Pediatrics. 2012;129(2):394-404.
5. Shelton TL, Stepanek JS. Excerpts from family-centered care for children needing specialized health and developmental services. Pediatr Nurs. 1995;21(4):362-364.
6. Fina DK, Lopas LJ, Stagnone JH, Santucci PR. Parent participation in thepostanesthesia care unit: Fourteen years of progress at one hospital. J Perianesth Nurs. 1997;12(3):152-162.
7. S. Singer GH, Marquis J, Powers LK, et al. A Multi-site Evaluation of Parent to Parent Programs for Parents of Children With Disabilities. J Early Interv. 1999;22(3):217-229.
8. Hemmelgarn AL, Glisson C, Dukes D. Emergency room culture and the emotional support component of family-centered care. Child Health Care. Published online 2001. https://www.tandfonline.com/doi/abs/10.1207/S15326888CHC3002_2
9. Solberg B. Wisconsin prenatal care coordination proves its worth: Case management becomes Medicaid benefit. Inside Preventive Care. 1996;2(3):1.
10. Griffin T, Abraham M. Transition to home from the newborn intensive care unit: applying the principles of family-centered care to the discharge process. J Perinat Neonatal Nurs. 2006;20(3):243-249; quiz 250-251.
11. National Survey of Children’s Health - Data Resource Center for Child and Adolescent Health. Accessed May 22, 2023. https://www.childhealthdata.org/learn-about-the-nsch/NSCH
12. 2021-NSCH-Methodology-Report.pdf.
13. Explore child mortality in the United States. America’s Health Rankings. Accessed July 15, 2023. https://www.americashealthrankings.org/explore/measures/child_mortality_a
14. Explore high health status - children in the United States. America’s Health Rankings. Accessed July 15, 2023. https://www.americashealthrankings.org/explore/measures/high_health_children
15. Tschudy MM, Raphael JL, Nehal US, O’Connor KG, Kowalkowski M, Stille CJ. Barriers to Care Coordination and Medical Home Implementation. Pediatrics. 2016;138(3). doi:10.1542/peds.2015-3458
16. General Pediatricians U.S. State and County Maps. American Board of Pediatrics. Accessed July 20, 2023. https://www.abp.org/dashboards/general-pediatricians-us-state-and-county-maps
17. Percent of children with a medical home. KFF. Published December 2, 2022. Accessed July 20, 2023. https://www.kff.org/other/state-indicator/children-with-a-medical-home/?currentTimeframe=0&selectedRows=%7B%22states%22:%7B%22arizona%22:%7B%7D,%22california%22:%7B%7D,%22kentucky%22:%7B%7D,%22massachusetts%22:%7B%7D,%22missouri%22:%7B%7D,%22new-mexico%22:%7B%7D,%22nevada%22:%7B%7D,%22texas%22:%7B%7D,%22rhode-island%22:%7B%7D,%22hawaii%22:%7B%7D%7D,%22wrapups%22:%7B%22united-states%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
18. Population distribution of children by race/ethnicity. KFF. Published October 28, 2022. Accessed June 2, 2023. https://www.kff.org/other/state-indicator/children-by-raceethnicity/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
19. Population distribution of children by race/ethnicity. KFF. Published October 28, 2022. Accessed July 20, 2023. https://www.kff.org/other/state-indicator/children-by-raceethnicity/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
20. Heath M, Hvass AMF, Wejse CM. Interpreter services and effect on healthcare - a systematic review of the impact of different types of interpreters on patient outcome. J Migr Health. 2023;7:100162.
21. US Census Bureau. Language use in the United States: 2019. Published online September 1, 2022. Accessed June 16, 2023. https://www.census.gov/library/publications/2022/acs/acs-50.html
22. Chen AH, Youdelman MK, Brooks J. The legal framework for language access in healthcare settings: Title VI and beyond. J Gen Intern Med. 2007;22 Suppl 2(Suppl 2):362-367.
23. CMS releases data briefs that provide key Medicaid demographic data for the first time. Accessed July 29, 2023. https://www.cms.gov/blog/cms-releases-data-briefs-provide-key-medicaid-demographic-data-first-time
24. Artiga S, Hill L, Damico A. Health coverage by race and ethnicity, 2010-2021. KFF. Published December 20, 2022. Accessed July 29, 2023. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity/
25. O’Dell ML. What is a Patient-Centered Medical Home? Mo Med. 2016;113(4):301-304.
26. CDC. Patient-centered medical home (PCMH) model. Centers for Disease Control and Prevention. Published May 14, 2021. Accessed July 28, 2023. https://www.cdc.gov/dhdsp/policy_resources/pcmh.htm
27. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780-781.
28. The SHARE Approach—achieving patient-centered care with shared decisionmaking: A brief for administrators and practice leaders. Accessed July 29, 2023. https://www.ahrq.gov/health-literacy/professional-training/shared-decision/tool/resource-9.html
29. Sepucha KR, Simmons LH, Barry MJ, Edgman-Levitan S, Licurse AM, Chaguturu SK. Ten Years, Forty Decision Aids, And Thousands Of Patient Uses: Shared Decision Making At Massachusetts General Hospital. Health Aff . 2016;35(4):630-636.
30. A to Z inventory - patient decision aids - Ottawa hospital research institute. Accessed November 5, 2023. https://decisionaid.ohri.ca/AZinvent.php
31. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4(4):CD001431.
32. Alston C, Qorvis MSLGROUP, Elwyn G, et al. Shared decision-making strategies for best care: Patient decision aids. NAM Perspect. 2014;4(9). doi:10.31478/201409f
33. Back AL, Fromme EK, Meier DE. Training Clinicians with Communication Skills Needed to Match Medical Treatments to Patient Values. J Am Geriatr Soc. 2019;67(S2):S435-S441.
34. Som M, Beaman J, Keener A, Stroup J. The Impact of Crucial ConversationsTM on Interpersonal Communication and Professionalism. OSMP. 2021;5(1). Accessed October 26, 2023. https://okstatemedicalproceedings.com/index.php/OSMP/article/view/149
35. Henderson S, Horne M, Hills R, Kendall E. Cultural competence in healthcare in the community: A concept analysis. Health Soc Care Community. 2018;26(4):590-603.
36. Fanta M, Ladzekpo D, Unaka N. Racism and pediatric health outcomes. Curr Probl Pediatr Adolesc Health Care. 2021;51(10):101087.
37. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42(2):727-754.
38. Driscoll A, Grant MJ, Carroll D, et al. The effect of nurse-to-patient ratios on nurse-sensitive patient outcomes in acute specialist units: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2018;17(1):6-22.
39. Mann S. Research shows shortage of more than 100,000 doctors by 2030. AAMC. Published December 31, 2018. Accessed September 20, 2023. https://www.aamc.org/news/research-shows-shortage-more-100000-doctors-2030
40. Chervoni-Knapp T. The Staffing Shortage Pandemic. J Radiol Nurs. 2022;41(2):74-75.
41. Shanafelt TD, West CP, Dyrbye LN, et al. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians During the First 2 Years of the COVID-19 Pandemic. Mayo Clin Proc. 2022;97(12):2248-2258.
42. Lucy CA, Wojtaszek J, LaLonde L, et al. Pediatrician Burnout Before and After the COVID-19 Pandemic. J Prim Care Community Health. 2023;14:21501319231194148.
43. Shaver J. The State of Telehealth Before and After the COVID-19 Pandemic. Prim Care. 2022;49(4):517-530.
44. McGrail KM, Ahuja MA, Leaver CA. Virtual Visits and Patient-Centered Care: Results of a Patient Survey and Observational Study. J Med Internet Res. 2017;19(5):e177.