| Characteristic | N = 177 |
|---|---|
| Year, n (%) | |
| 2018 | 28 (15.82) |
| 2016 | 23 (12.99) |
| 2017 | 21 (11.86) |
| 2019 | 21 (11.86) |
| 2022 | 16 (9.04) |
| 2014 | 15 (8.47) |
| 2015 | 14 (7.91) |
| 2020 | 14 (7.91) |
| 2021 | 11 (6.21) |
| 2023 | 8 (4.52) |
| 2013 | 6 (3.39) |
| Phase, n (%) | |
| 3 | 127 (71.75) |
| 4 | 50 (28.25) |
| Continent, n (%) | |
| Multiple | 75 (42.37) |
| Europe | 41 (23.16) |
| Asia | 34 (19.21) |
| North America | 20 (11.29) |
| Africa | 3 (1.69) |
| Australia | 3 (1.69) |
| South America | 1 (0.56) |
| Recruitment Status, n (%) | |
| Completed | 56 (31.64) |
| Recruiting | 43 (24.29) |
| Unknown | 22 (12.43) |
| Terminated | 21 (11.86) |
| Active, but No Recruiting | 17 (9.60) |
| Not Yet Recruiting | 10 (5.65) |
| Withdrawn | 6 (3.39) |
| Enrolling by Invitation | 1 (0.56) |
| Suspended | 1 (0.56) |
| Funding Type, n (%) | |
| Industry | 93 (52.54) |
| Multiple Without Industry | 30 (16.95) |
| Hospital | 24 (13.56) |
| University | 14 (7.91) |
| Multiple With Industry | 13 (7.34) |
| Private | 3 (1.69) |
| Enrollment Number, Median (IQR) | 196 (84 – 482) |
| Trial Duration in Months, Median (IQR) | 38 (26 – 64) |
| Type of Intervention, n (%) | |
| Biologics | 64 (36.16) |
| Multiple | 51 (28.81) |
| Other | 42 (23.73) |
| Immunosuppressant | 13 (7.34) |
| Aminosalicylates (ASA) | 5 (2.82) |
| Corticosteroids | 2 (1.13) |
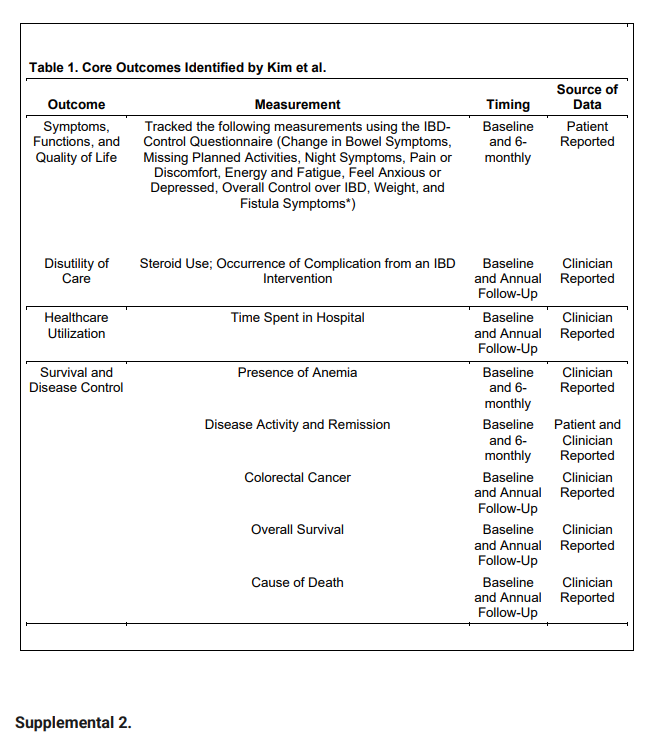
| Domain | Outcome Set Item | N = 177 |
|---|---|---|
| Symptoms, Function, and Quality of Life | Change in Bowel Symptoms, n (%) | |
| Yes | 156 (88.14) | |
| No | 21 (11.86) | |
| Missing Planned Activities, n (%) | ||
| Yes | 76 (42.94) | |
| No | 101 (57.06) | |
| Night Symptoms, n (%) | ||
| Yes | 57 (32.20) | |
| No | 120 (67.79) | |
| Pain or Discomfort, n (%) | ||
| Yes | 147 (83.05) | |
| No | 30 (16.95) | |
| Energy and Fatigue, n (%) | ||
| Yes | 75 (42.37) | |
| No | 102 (57.63) | |
| Feel Anxious or Depressed, n (%) | ||
| Yes | 78 (44.06) | |
| No | 99 (55.93) | |
| Overall Control Over IBD, n (%) | ||
| Yes | 109 (61.58) | |
| No | 68 (38.42) | |
| Weight, n (%) | ||
| Yes | 94 (53.11) | |
| No | 83 (46.89) | |
| Symptoms, Function, and Quality of Life (Crohn's) | Fistula Symptoms, n (%) | |
| Yes | 19 (21.8) | |
| No | 68 (78.2) | |
| Not Applicable | 90 | |
| Disutility of Care | Steroid use, n (%) | |
| Yes | 64 (36.16) | |
| No | 113 (63.84) | |
| Occurrence and Impact of Complication From an IBD Intervention, n (%) | ||
| Yes | 69 (38.98) | |
| No | 108 (61.02) | |
| Healthcare Utilization | Time Spent in Hospital, n (%) | |
| Yes | 43 (24.29) | |
| No | 134 (75.71) | |
| Survival and Disease Control | Presence of Anemia, n (%) | |
| Domain | Outcome Set Item | N = 177 |
| Yes | 57 (32.20) | |
| No | 120 (67.79) | |
| Disease Activity and Remission, n (%) | ||
| Yes | 146 (82.49) | |
| No | 31 (17.51) | |
| Colorectal Cancer, n (%) | ||
| No | 177 (100.00) | |
| Overall Survival, n (%) | ||
| Yes | 2 (1.13) | |
| No | 175 (98.87) | |
| Cause of Death, n (%) | ||
| Yes | 15 (8.47) | |
| No | 162 (91.53) |
| Characteristic | N = 1771 | F-statistic2 | p-value2 | (η2)2 |
|---|---|---|---|---|
| Continent | 4.79 | <0.001 | 0.14 | |
| Africa | 33.09 (19.50) | |||
| Asia | 28.09 (18.38) | |||
| Australia | 37.87 (13.09) | |||
| Europe | 38.66 (22.03) | |||
| Multiple | 48.84 (22.04) | |||
| North America | 44.49 (15.22) | |||
| South America | 5.88 (NA) | |||
| Funding Type | 3.37 | 0.01 | 0.09 | |
| Hospital | 36.73 (22.86) | |||
| Industry | 46.32 (22.36) | |||
| Multiple With Industry | 34.47 (17.83) | |||
| Multiple Without Industry | 30.37 (19.79) | |||
| Private | 54.04 (11.92) | |||
| University | 42.91 (15.61) | |||
| Recruitment Status | 1.82 | 0.08 | 0.08 | |
| Active, but No Recruiting | 46.47 (19.60) | |||
| Completed | 47.45 (21.81) | |||
| Enrolling by Invitation | 41.18 (NA) | |||
| Not Yet Recruiting | 35.15 (22.49) | |||
| Recruiting | 37.40 (21.51) | |||
| Suspended | 68.75 (NA) | |||
| Terminated | 40.72 (21.37) | |||
| Unknown | 30.98 (21.06) | |||
| Withdrawn | 43.01 (23.37) | |||
| Characteristic | t-statistic3 | p-value3 | (r)3 | |
| Enrollment Number | 3.24 | 0.001 | 0.24 | |
| 1Mean (SD) | ||||
| 2One-way ANOVA, η2 | ||||
| 3Pearson Correlation Coefficient |