| Study Characteristics | Kerr et al.6 | Simon et al.7 | Mannes et al.9 |
|---|---|---|---|
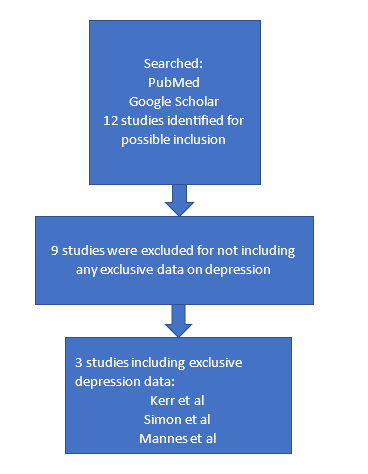
| Study title | Current Physical and Mental Health of Former Collegiate Athletes | Health-Related Quality of Life in Former National Collegiate Athletic Association Division I Collegiate Athletes Compared with Noncollegiate Athletes: A 5-Year Follow-up | Prevalence and Correlates of Psychological Distress among Retired Elite Athletes: A Systematic Review |
| Participants | 421 female and 376 male former athletes | 128 male and 65 female former athletes and 80 male and 89 female non-collegiate athletes | 40 articles were included for review |
| Interventions | online, self-reported questionnaire compared to normative U.S. data collections | online, self-reported survey PROMIS with demographics questionnaire | articles included self-reported surveys as well as clinical diagnoses |
| Inclusion and exclusion criteria | Inclusion: 18 years or older, had an email address from the university alumni association, able to speak and understand English,and played at least one season of collegiate sport between 1972-2012 Exclusion: incomplete data from survey | Inclusion: former Division I athlete, date of birth as used for inclusion criterion as well, participants who attended the university,but did not participate in sanctioned athletics. Exclusion: volunteers who did not complete the full survey | Inclusion: retired collegiate or professional athletes, had to have played for at least one year at either level,inclusion for articles: English language, published peer-review journals, and quantitative studies Exclusion: studies examining cognitive impairment exclusively |
| Outcome measures | t-tests were used to compare PCS and MCS health composite scores between participants and the World Health Organization U.S. population data | Descriptive statistics, Cohen's d effect sizes, repeated measures multivariate analysis of variance, university analyses of variance, t tests, chi-square analysis, and a T-score metric were used for different parts of the study results. For the PROMIS scales, they used Shapiro-Wilk tests that were assessed by box plots. | Mixed Method Appraisal tool for evaluation bias. 21 articles measured depression rates, and 13 articles compared to results to non-athletes. |
| Results | They found that the MCS and PCS scores were similar between former collegiate athletes and the US population, and prevalent medical conditions in former athletes included anxiety, hypercholesterolemia/high cholesterol, and depression. | They found significantly higher scores for depression, fatigue, pain, and physical function scores compared to the non-collegiate population. | It was found that there was a higher prevalence rate when studies used a psychologist or psychiatrist to diagnose depression vs. self-reported data. From the articles, they also found that with greater physical activity, depression rates decreased. They also reported that there is a lack of care for former athletes’ mental health once they end their careers. |
| Level of evidence | 3 | 2 | 1 |
| Evidence quality score | 19/22 | 21/22 | 18/22 |
| Support for the answer | Yes | Yes | Yes |