Abstract:
An oropharyngeal lipoma is a rare benign tumor comprised of adipose tissue found in the tissues of the upper aerodigestive tract. While non-cancerous and slow-growing, these masses can enlarge to cause symptoms such as dyspnea, voice changes, and shortness of breath. Complications of large, tubular oropharyngeal lipomas can include prolapse into the oral cavity, leading to airway obstruction. We present the case of a 62-year-old male with an unknown medical history who was diagnosed with an oropharyngeal lipoma following protrusion of the mass through his oral cavity after a coughing fit. This case highlights the importance of prompt diagnosis and definitive treatment with surgical excision to relieve symptoms and eliminate the imminent risk of airway compromise and death.
Key Words: Neuroradiology, oropharynx, lipoma, airway, otolaryngology, case report.
Introduction :
Lipomas, known as the “universal tumor” because of their ability to occur throughout the body, are the most common soft tissue tumors; however, those located in the upper respiratory and digestive tracts are rare, accounting for less than 5% of all benign tumors of the oropharynx and oral cavity. 1,2 The classic CT appearance of lipomas demonstrates well-defined, homogenous lesions with low attenuation of -65 to -125 Hounsfield Units. 2 Lipomatous lesions have a soft and mobile composition, predisposing patients to the risk of prolapse into the oral cavity when oropharyngeally located, typically occurring following a coughing fit. This usually unexpected prolapse can lead to potentially lethal complications, including airway compromise and total obstruction during anesthesia induction. Due to the slow-growing nature of lipomas, many case reports of similar lesions note chronic symptoms occurring for years before complications and eventual diagnosis. Some cases of oropharyngeal lipomas remain asymptomatic until they are incidentally found on imaging.
Differential diagnoses for oropharyngeal lesions include laryngeal lipomas, malignant masses, mucous retention cysts, and dermoid or epidermoid cysts. 2 Liposarcomas can also appear similarly on imaging. These etiologies can be differentiated through a combination of physical exam findings, imaging, and biopsy, often requiring microscopic evaluation to screen for atypical, malignant cells. MRI may help differentiate between benign and atypical, or malignant, lipomas. Benign lipomas tend to be smaller in size with higher fat content, fewer or absent septations, and absent or minimal enhancement. 3
We present a case involving a 62-year-old male with an unknown past medical history, who was diagnosed with an oropharyngeal lipoma. Prompt evaluation and surgical excision led to successful recovery and a lack of known recurrence, illustrating the effectiveness and importance of surgical treatment to improve long-term patient outcomes.
Case presentation:
A 62-year-old male with an unknown past medical history was evaluated in the emergency department with impending airway compromise due to an undetermined, irreducible oropharyngeal mass expelling from the patient’s mouth after a severe coughing fit. The patient was unable to speak upon presentation and was unable to maintain his airway while lying flat. No prior similar episodes had been experienced by the patient, but he did note a history of difficulty swallowing for many years.
The patient was quickly transferred to the OR following recommendations by general surgery, ENT, and anesthesia, where he was successfully orally intubated under general anesthesia. A large, tubular, soft tissue mass with a smooth mucosal surface was noted in the right piriform sinus, extending through the oral cavity past the teeth, and occupying a large portion of the oropharynx. Following surgical exploration of the mass, vocal cords, arytenoids, epiglottis, and glottis, the patient remained intubated and was transferred to the ICU in stable condition.
A non-contrast CT of the head and neck showed a large homogenous mass extending from the patient’s oropharynx with a fat density (Figs. 1-4). The patient was then transferred to another hospital in the community for direct laryngoscopy and surgical excision of the oropharyngeal mass. Surgical excision showed a large, soft, well-circumscribed, pedunculated mass greater than 6 centimeters extending from the left posterior cricoid region out of the oral cavity (Figs. 5-7). The remaining airway appeared normal. An acute maxillary sinus infection was also suspected due to purulent discharge draining from the nasopharynx appreciated both grossly and with diagnostic rigid nasal endoscopy.
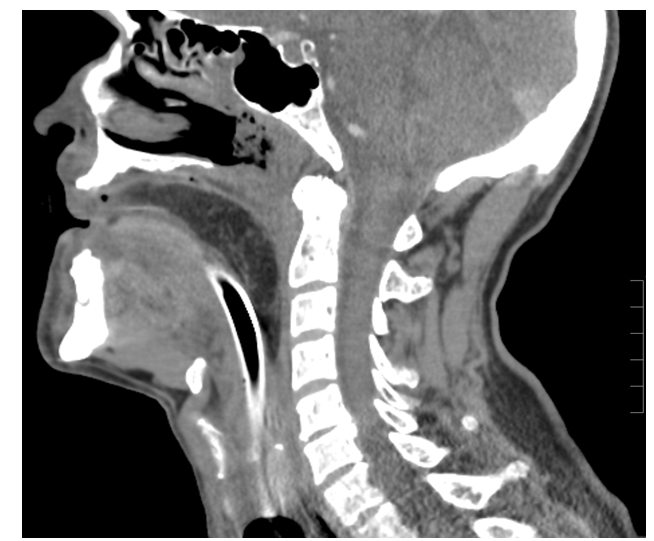
Figure 1. Non-contrasted, sagittal CT of the head and neck demonstrating a large oropharyngeal mass of fat density. There is slight extension into the hypopharynx and an endotracheal tube coursing beneath the mass.
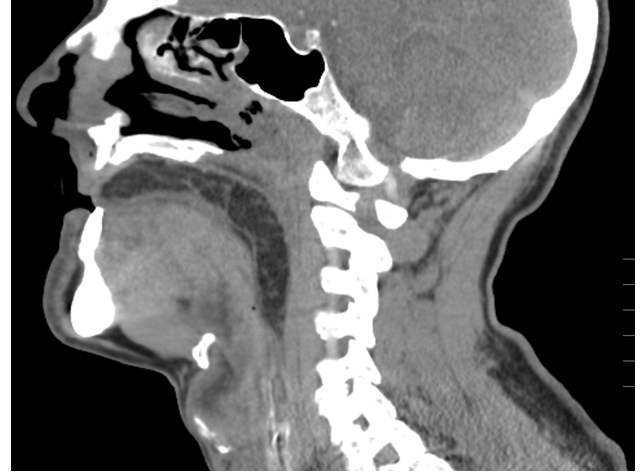
Figure 2. Non-contrasted, sagittal CT of the head and neck redemonstrating a large oropharyngeal mass of fat density with hypopharyngeal extension. Endotracheal tube is not visualized as it was placed in a right inferolateral position in relation to the mass.

Figure 3. Non-contrasted coronal CT of the head and neck demonstrating a large oropharyngeal mass of fat density. Endotracheal and enteric tubes are visualized coursing in a right inferolateral position in relation to the mass.

Figure 4. Non-contrasted axial CT of the head and neck demonstrating a large oropharyngeal mass of fat density. Endotracheal and enteric tubes are visualized coursing lateral to the mass.



The mass was sent for pathology examination and report, which demonstrated atypical cells, and FISH molecular testing was conducted. Grossly, the specimen consisted of a 9.0 x 4.2 x 2.8-centimeter oblong mass that was encapsulated and vascularized with a tan-gray mucosal surface with purulent material. The mucosal surface was thickened up to 0.3 centimeters. Once serially sectioned, pale yellow lobulations were appreciated. Positive and negative immunohistochemical, molecular probing, immunofluorescence, and other histochemical controls were examined with appropriate staining. Immunohistochemical testing resulted negative for MDM2 staining on all slides. The samples were not amplified when evaluating the MDM2/CEP12 FISH ratios. Lack of amplification signifies lower suspicion for atypical lipomatous tumors or well-differentiated liposarcomas. It was determined that the mass was comprised of mature adipose tissue, most consistent with a benign lipoma.
Discussion:
Lipomas can vary greatly in size, with superficial lipomas typically measuring less than 5 centimeters and deep lipomas having the ability to grow to over 20 centimeters in size. 4 The case presented in this report describes an impressively large lipoma with a length of 9.0 centimeters. The largest oropharyngeal lipoma published at the time of this writing was measured at 17 centimeters in length, making this case the second largest oropharyngeal lipoma reported thus far. 5 Surprisingly, the patient with the largest reported oropharyngeal lipoma denied experiencing any symptoms before a coughing attack resulting in protrusion of the mass through the patient’s mouth. As previously mentioned, presenting symptoms can include voice changes, dysphagia, sensations of throat fullness, and shortness of breath when lying prone. Electrolyte imbalances and dehydration can result from these potentially uncomfortable symptoms of a growing mass, especially in geriatric patients. 1 Potential prolapse of these lipomas is dangerous, as it can lead to airway compromise, and even death, caused by laryngeal obstruction from pedunculated lipomas at the epiglottis, aryepiglottic fold, or posterior cricoid. 6
In order to prevent total airway obstruction during anesthesia, awake fiberoptic intubation (AFOI) should be considered following careful assessment of the airway. 2 AFOI is regarded as the gold standard for managing a known or anticipated difficult airway. It allows for direct visualization of airway structures while maintaining spontaneous breathing, decreasing the risk of aspiration or tube impingement.
Although MRI is generally considered superior to CT when evaluating soft tissues and tumor extension, MRI is less accessible, more costly, and more time-consuming, resulting in CT functioning as the primary mode of diagnosis for most oropharyngeal lipomas. 3 CT cannot, however, reliably differentiate between a benign lipoma versus a malignant liposarcoma, further emphasizing the importance of obtaining tissue samples or performing mass excision of the growing lesion.
Essential treatment includes complete surgical excision. 6 As in this case, prompt surgical excision resulted in immediate and complete resolution of symptoms. If the capsule is excised without disruption of its integrity, the recurrence rate is less than 5% for lipomas over time. 4 Therefore, the prognosis for this presentation is excellent, but long-term follow-up is recommended due to the possibility of a missed diagnosis of liposarcoma. 5 Combining the use of physical exam findings, imaging, and biopsy can aid in definitive diagnosis and proper management.
Conclusion:
This case highlights the rarity and sudden danger that a slow-growing oropharyngeal lipoma can impose. Informative imaging of potential oropharyngeal lipomas is essential for not only the diagnosis of the lesion, but also for anesthetic and surgical planning. Prompt diagnosis followed by surgical excision is crucial for symptomatic management and avoiding life-threatening complications. Despite such a sudden and dangerous presentation of an oropharyngeal lipoma in the case presented, expeditious evaluation, diagnosis, and treatment among the emergency department physicians, radiologists, anesthesiologists, otolaryngologists, and pathologists allowed for a potentially life-saving intervention for the patient. Awareness of similar patient presentations is critical for proper recognition and management of future cases of oropharyngeal lipomas.
References:
1. Akın V, Okur E, Kumbul YÇ, Okur N, Kum R. Oral Lipoma Resembling Popeye's Pipe: A Case Report. Cureus 2022;14(2):e22350. https://doi.org/10.7759/cureus.22350
2. Lunn J, Mathew R, Modayil P. Oropharyngeal lipoma; a rare and dangerous cause of voice change. BMJ Case Reports 2019;12(7):e230161. https://doi.org/10.1136/bcr-2019-230161
3. Knipe H, Silverstone L, Anan R, et al. Lipoma vs well-differentiated liposarcoma. Radiopaedia.org 2019. https://doi.org/10.53347/rID-68800
4. Gaillard F, Walizai T, Paládi B, et al. Lipoma. Radiopaedia.org 2009. https://doi.org/10.53347/rID-7654
5. Mitchell JE, Thorne SJ, Hern JD. Acute stridor caused by a previously asymptomatic large oropharyngeal spindle cell lipoma. Auris Nasus Larynx 2007;34(4):549-552. https://doi.org/10.1016/j.anl.2007.02.001
6. Tan KS, Jalaluddin WMS, Lipoma of vallecula—a case report. BJR Case Reports 2016; 2(3)20150460. https://doi.org/10.1259/bjrcr.20150460