Improving Surgical Efficiency: An Evidence-Based Approach to Reducing Incidence of Last-Minute Case Cancellation
Samuel J. Huber, MHA, PMP
Oklahoma State University Center for Health Sciences
samuel.huber@okstate.edu
No funding was received in support of this work.
No conflicts of interest exist for this author.
Abstract
Unplanned cancellation of surgery in the final hours preceding case start time causes significant disruption within surgical settings. Often, last-minute surgical cancellation results in unutilized operating room time. In these instances, healthcare organizations continue to incur overhead costs while forfeiting potential revenue. Additionally, last-minute cancellation of surgery is associated with a measurable decline in patient outcomes, including greater risk of hospital admission and mortality. The incidence of unplanned surgical cancellation is a formidable issue that affects health systems of all sizes within the United States. A literature review was conducted to identify evidence-based solutions to mitigate this health system challenge. Three primary interventions were identified through analysis of current research: optimization of preoperative services, process improvement through Lean Six Sigma, and integration of mobile health technology. These solutions were evaluated using a framework of best practices in public health impact. Optimization of preoperative services, with an emphasis on nurse-led programs, emerged as the ideal strategy due to its overall effectiveness, feasibility, and sustainability. Preoperative clinics have the potential to further reduce surgical cancellations by expanding the range of services offered. Additional exploration of available services in the preoperative period may serve to maximize the impact of this strategy for both patients and healthcare organizations.
Introduction
As a cornerstone of modern medicine, surgical care plays a critical role in driving both the financial structure of health systems and the clinical outcomes of the patients they serve. Throughout the world, more than 300 million surgical procedures are performed each year 1. Of these, some 64 million occur within the borders of the United States, accounting for greater than 20% of global surgeries 2. Intervention within the operating room (OR) has become a foundational element to acute, intensive, and elective care in the present era of medicine. For every four hospital admissions occurring in the United States, one or more involve some degree of surgical care 3, 4.
Surgical procedures are performed in a variety of facility types within the healthcare realm. Patients today may receive surgical care within the inpatient hospital setting, outpatient hospital-based surgical units, ambulatory surgery centers (ASCs), or even within specialty physician clinics. The Association of American Medical Colleges (AAMC) reports that as of 2022, there are 155,549 practicing surgeons within the country 5. These physicians provide surgical care to an estimated 37 million Americans each year, or approximately one in nine citizens 6.
The revenues and costs generated from operative care are monumental to the financial structure of the national health system. Measuring public expenditure, payments made for surgical services account for greater than 50% of the $829 billion that Medicare spends annually on service reimbursement 7, 8. The influence of surgery-related finance extends heavily into the budgets of health systems as well. The OR accounts for as much as 40% of hospital costs, and generates between 60% and 70% of net hospital revenues 9. In one year, a single general surgeon may bring in $2.7 million in revenue to their hospital system, while other specialty surgeons such as orthopedic and cardiovascular surgeons can produce greater than $3 million in annual revenue 10. The outstanding impact of surgical services on hospital revenue makes OR utilization and efficiency a critical aspect of organizational planning.
This massive revenue stream is respectively countered by a high-dollar cost structure within the OR. A study of both inpatient and ambulatory surgical sites in the state of California found that the average cost of a functioning OR is $36 to $37 per minute 11. The study investigated contributing elements of the cost structure, and ultimately determined that less than 10% of operating expenses were created by supplies consumed on a variable basis. A separate review concluded that nationally, the average cost created by an OR was $46.04 per minute 12. Both studies identified large overhead costs as a limitation in producing an accurate figure, leading to variance in their final estimates. Ultimately, the OR generates revenue only when surgical services are performed, yet the cost structure is predominantly fixed. The result of this is a system in which unutilized OR time causes a loss in revenue, while health systems continue to incur appreciable cost 13.
Time in the OR goes unutilized if surgeries go unscheduled, or when scheduled procedures are cancelled without timely replacement, as often occurs with last-minute case cancellation. A multitude of studies have investigated the incidence of surgical cancellation throughout varying service lines. One analysis of last-minute cancellation of arthroscopic surgeries at an ASC found that 2.7% of procedures were cancelled within the final 24 hours of case start time 14. A separate study at one academic health center found that 4.4% of surgeries were cancelled on the day of the procedure, and identified that 71.6% of these were related to a “potentially avoidable” cause 15. Over a four-year period in one medium-sized tertiary hospital, an estimated 14% of 20,881 procedures were cancelled, with 83.5% of those being related to an administrative or system-centered error 16. Another study concluded that 3.1% (121 of 3,904) of surgical services were cancelled on the day of the case at a 700-bed teaching hospital 17. Despite variance in magnitude among different facility types, numerous studies have identified last-minute cancellation of surgery as an immediate challenge for health systems’ success across the board.
Problem Statement
The burden of last-minute surgical cancellation can be measured in both patient outcomes and system performance metrics. In a retrospective review of 41,389 cases scheduled at a large academic medical center, 17.1% (36) of patients who experienced same-day cancellation required hospital admission within 30 days, and 1.9% (4) of patients died within the same timeframe 18. It has also been found that in patients affected by surgical cancellation, 42% report worsening physical condition, 48% report heightened emotional strain, and 28% report an increased need for pain controlling medication 19. On the operational side, idle OR time incurs an estimated cost of $2,040 per hour, and underutilization of as little as 15% of the OR schedule may result in revenue losses of up to $60,256 per week 11, 13. With impacts reaching into health system finance and clinical care outcomes, last-minute surgical cancellation is a critical challenge in health administration that warrants further investigation into contemporary solutions.
Research Question
The complexity of this health system challenge necessitates research that is both targeted and solution oriented. The ECLIPSE framework was selected as the most practical model for driving meaningful, effective research for this literature review. Figure 1 below details the components of the ECLIPSE framework, as well as a brief description of their role in this health system topic.
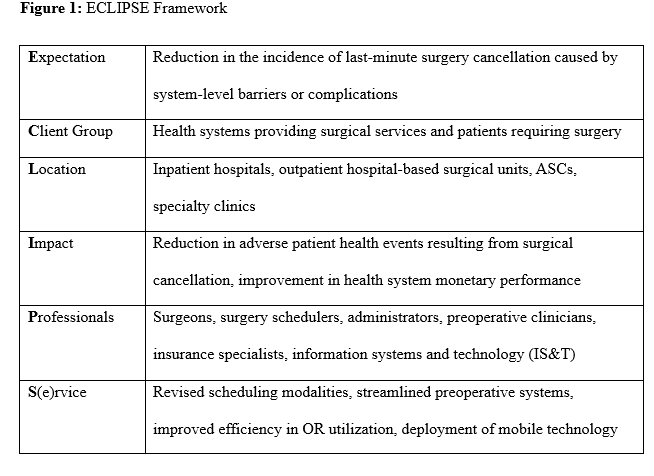
With consideration to the magnitude of the issue as well as the challenges in addressing it, the ECLIPSE framework was utilized in developing the following research question: What interventions can health systems in the United States implement to reduce the incidence of last-minute surgical case cancellation?
Expectation
A review of over 6,000 surgical cases from 25 health centers across various settings found that same-day cancellation rates of 10% or greater were common 20. The expectation in this framework is identification of strategies that health systems can reasonably implement to lower the incidence of preventable case cancellation.
Client Group
Successful findings may provide value to both healthcare organizations and the patient populations they serve. Unutilized OR time generates preventable costs as well as loss of potential revenue. On the patient side, the scale of the issue consists of an estimated 37 million Americans who receive surgical care each year 6.
Location
Operative procedures are conducted within a range of settings, including inpatient surgical units, outpatient hospital-based surgical facilities, ASCs, and specialty physician offices. Non-clinical resources that support the surgical service line, such as scheduling and access, are often located within the same facility as the operating space.
Impact
Last-minute case cancellation contributes to preventable risk of patient health and safety events. Same-day cancellation is associated with increased incidence of hospital admission and mortality 18. Implementation of structural initiatives to reduce cancellation may lead to improved patient outcomes and reduced surgical wait times 21. The scope of the impact additionally reaches into the financial performance of healthcare organizations that perform procedures. Surgical departments incur operating losses of more than $2,000 per hour for idle OR time 11.
Professionals
The provision of surgical care is a multidisciplinary effort that requires ongoing collaboration between a vast network of professionals. While surgeons are responsible for performing the key components of procedures, they receive clinical support from anesthesiologists, residents, surgical technicians, nurses, and other patient-facing staff. The service line is supported by schedulers, IS&T professionals, claims agents, and medical coders. Both clinical and non-clinical teams rely on the dedicated leadership of health administrators.
Service
The challenge of reducing last-minute surgery cancellation is not one dimensional. Procedures are pushed back or removed entirely for a range of reasons, including system-level errors, insurance barriers, clinical complications, and patient attendance failures 16. Successful interventions may take the form of improved scheduling modalities, enhanced preoperative protocols, revised OR efficiency strategies, or technological innovations.
Logic Model
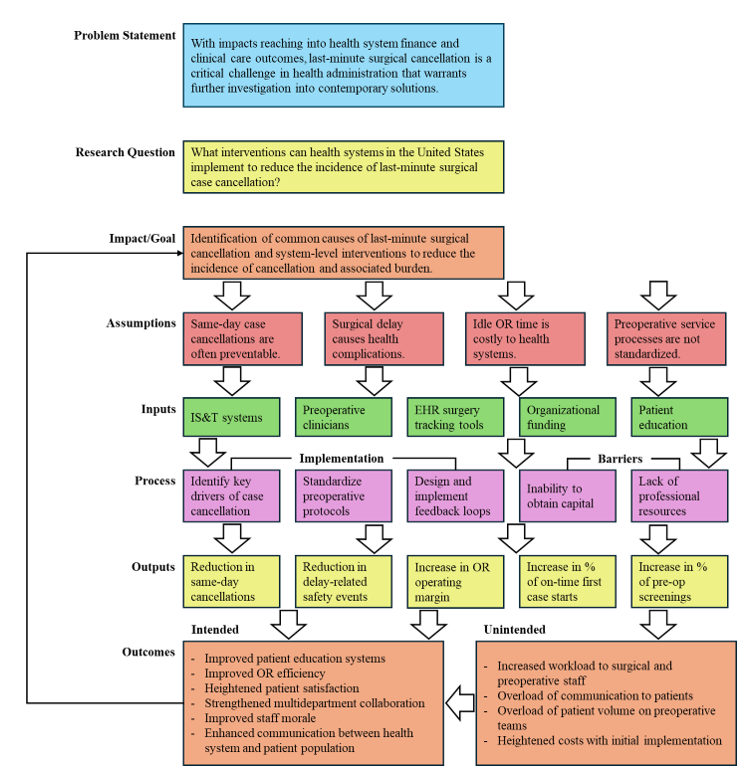
A comprehensive framework that considers modern and relevant health system factors is imperative to effectively address the research question. The logic model depicted in Figure 2 was designed as a foundational tool to produce well-rounded, practical solutions to the health system challenge of late surgical cancellation. This model analyzes key assumptions, inputs, implementation processes, implementation barriers, outputs, and outcomes – both intended and unintended. A visual of the applied logic model is seen below, in Figure 2.
Figure 2: Logic Model
Methods
Throughout the literature review addressing this health system challenge, resources were obtained through the University of Cincinnati Library system, as well as databases including PubMed, EBSCOhost, and Google Scholar. Searches for peer-reviewed, primary studies were conducted using key phrases such as “reducing surgical cancellation”, “last-minute surgery cancellation”, “same-day surgery cancellation”, “operating room efficiency”, “preoperative clinic cancellation”, and “interventions to reduce cancellation”. Results were limited to the past ten years to ensure that only current, relevant studies were utilized. Preference was given to randomized controlled trials and cohort studies. Noteworthy journals of focus included The American Journal of Surgery, International Journal of Surgery, Journal of Anesthesia, and International Journal for Quality in Health Care. In total, 22 resources were selected for this literature review. Selection of studies was driven by their relevance to the health system challenge, external validity of findings, and analysis of distinct interventions. Due to the nature of these interventions, many of the studies collected both prospective and retrospective patient data. All articles selected, with the exception of one, were primary research studies. The single exception was an implementation narrative evaluating the process and efficacy of developing a new technological intervention. Two of the selected studies were doctoral dissertations. One of these did not explicitly state its sample population size. The author of one study was contacted via email for further information on their methods and findings 22.
Literature Review
This literature review was guided by the ECLIPSE framework research question. Utilizing the selected sources, three strategies to reduce last-minute surgical case cancellation are proposed. Current evidence indicates that optimization of preoperative services, process improvement through Lean Six Sigma, and integration of mobile health technology are all viable interventions to mitigating this systemic health challenge.
Optimization of Preoperative Services
The interval between surgery scheduling and date of service constitutes a preoperative window in which potentially avoidable causes of last-minute case cancellation can be systematically identified and addressed. During this preoperative window, health organizations have the opportunity to verify insurance authorization, assess patient educational needs, complete health examinations, and confirm patient understanding of surgical plans 23. Oversight of this critical period contributes to preventable causes of same-day case cancellation. In its current state, the American health system lacks standardization across preoperative services. One retrospective cohort analysis exemplifies this, reporting that in 63 Midwest hospitals of varying size, limited preoperative standardization was a key driver of cancellations within surgical facilities 24.
Evidence from current literature suggests that optimization of standardized preoperative clinics promotes early identification of complications, which in turn reduces the incidence of last-minute surgical cancellation.
Preoperative assessment with a focus on anesthesia considerations represents one evidence-based method for optimizing services. One study demonstrated the success of a preoperative anesthesia clinic (PAC) utilizing telehealth services for standardized screenings 25. This prospective quality improvement project analyzed same-day cancellation incidence in 2,189 surgeries across a 12-week period, consisting of six weeks of pre-PAC cases and a six-week post-PAC interval. Ultimately, date of service cancellation fell from 3.38% to 1.72% following the development of the PAC. Another study of PAC implementation documented a retrospective analysis of surgical cancellations over an 11-year period, comparing the incidence before and after the implementation of a PAC 26. Throughout the duration of the study, 48,089 surgical cases were cancelled. Incidence of cancellation following the development of the PAC was reduced by 56.9% (0.051 to 0.022). A separate study sought to evaluate the impact of leadership from an attending anesthesiologist in the preoperative clinic 27. In a one-year analysis of more than 50,000 cases, both pre and post intervention, cancellation rate decreased from 3.1% to 2.6%. The study further evaluated potential cost savings to the organization, estimating an impact between $230,000 to $300,000 throughout the duration of the study.
Department specific preoperative services represent another viable mechanism to reduce cancellation. An ambulatory driven approach investigated the utilization of clinical office staff in preoperative preparation 28. The authors conducted a six-month retrospective review followed by a six-month post-intervention analysis. In the intervention phase, ambulatory staff contacted patients four days prior to their date of service to confirm surgery time, preoperative instructions, review health history, and answer patient questions. Among the 5,838 cases examined in the study, last minute cancellation fell from 12% to 11.8%. A separate study focused on urology-specific preoperative screenings assessed the intervention’s impact on cancellation across 949 cases 29. Screenings targeted department specific cancellation factors, such as urinary tract infection in the preoperative window. Early screenings created opportunities for clinicians to proactively address clinical barriers, primarily through the provision of antibiotics for infections. These efforts were associated with a reduction in cancellation rate from 23.9% to 4.3% over the course of six months.
Another well-studied approach to optimization of preoperative services is the nurse-led clinic. Pediatric cases in one ambulatory surgery center were evaluated over a three-month period following the creation of a nurse-led call program 30. In this prospective cohort analysis, patients and their guardians were contacted a minimum of two times within the final 14 days leading to surgery. During these communications, clinicians reviewed critical education, confirmed health history, and allotted time for patient questions. The intervention, which was applied to 310 cases, was associated with a reduction in cancellation incidence from 16.8% to 8.8%. Another nurse-led clinic, a preoperative “One-Stop Shop”, was implemented and evaluated for success in a suburban community hospital 31. This highly standardized intervention utilized a checklist tool on approximately 500 cases per month, which contributed to a same-day cancellation rate reduction from 10% to 3%. The study additionally identified a 1% improvement to patient experience, and a 5% improvement to staff engagement. The financial impacts of nurse-led preoperative clinics have documented evidence of success. A one-year study of retrospective and prospective cancellation data from a four-room ophthalmology surgery site presented cost-benefit analysis of a nurse-led clinic, and approximated a 61% annual return on investment 22.
A more comprehensive approach to effective utilization of the preoperative window may be achieved through the formation of a multidisciplinary clinic. In this setting, nurses, anesthesiologists, dentists, and pharmacists collaborate to ensure that each facet of preoperative screening is appropriately performed. The impact of such a clinic was studied throughout a six-month intervention period at one academic hospital, with findings compared to a six-month pre-intervention period 32. Among the 8,862 patients included in the study, case cancellation was 31.9% lower among patients who received preoperative assessment from the multidisciplinary clinic. Additionally, the study asserted that last-minute cancellation related to preventable causes, including authorization and medication compliance, was 42.9% lower in the intervention group.
Evidence supports the utility of optimizing preoperative services with standardized screening modalities. This has been successfully accomplished in varying surgical settings through the implementation of PACs, department specific programs, nurse-led clinics, and multidisciplinary preoperative clinics.
Process Improvement Through Lean Six Sigma
A discernible margin of last-minute surgical cancellation is rooted in system-level error. Deficiencies in accurate, reliable processes that are beyond patient control have been found to contribute to case cancellation. At one academic hospital, a prospective audit of 5,929 cases labeled 71.6% (187) of all same-day cancellations as “potentially avoidable” by the health system 15. Of these “potentially avoidable” cancellations, nearly 80% (150) were attributed to incomplete financial authorization, insufficient medical workup, failure of patient to appear, and delays in the OR schedule. A highly adopted methodology to combat these challenges is the Lean Six Sigma (LSS) framework. This tool is used by administrators, physicians, and process improvement professionals within healthcare systems to reduce variability in outcomes and minimize process waste 33.
LSS has applications in department and field specific initiatives to improve surgical processes. One study applied the methodology to the cardiac surgery department of an academic hospital that was experiencing abnormally high cancellation incidence (~20%) in cardiac cases 34. The study collected 20 months of retrospective data and 16 months of post-intervention data for coronary artery bypass graft cancellation. Interventions developed as a result of process improvement through LSS included: smart OR scheduling, a new check-in process, dedicated intensive care unit (ICU) beds, and a fast-track ICU. The number of last-minute cancellations per month decreased from 16 (19%) to 8 (5%) over the duration of the study. A 2021 study of LSS application in the orthopedic surgery department at a large private hospital evaluated the impact in reducing error and variability 35. The organization provided LSS training to more than 250 employees. A dedicated LSS team was established to improve surgical processes, and developed the goal of achieving 90% “right first time” in surgery scheduling. Following a six-month intervention deployment period, the team evaluated orthopedic surgeries in a three-week post-intervention period, which concluded that 100% (30) surgeries had been scheduled “right first time”.
The methodology can be applied to larger components of health systems beyond single departments or single service lines. Implementation of the LSS framework was studied throughout all surgical divisions at a large tertiary hospital 36. Over a 12-month period, LSS was utilized to identify key drivers of last-minute cancellation and develop new processes. During the first quarter of study, 12.3% (775) of surgeries were cancelled. Throughout the final quarter, the cancellation rate had been reduced to 4.67% (278). The cancellation rate remained below 5% for the following three years until the publication of the study.
Improvement to on-time first case start is an additional outcome that has been investigated with respect to LSS. Delays in first case start time are associated with increased cancellation of afternoon surgeries and additional hospital costs of up to $400,000 annually 37. The impact of a multidisciplinary committee utilizing LSS to improve first case on-time starts was studied over a 20-month period 38. Within 12 months of intervention, on-time starts increased from 30% to 79%, and surgical delays were reduced by 49%. A 2017 study implemented interventions to the surgery department of a large academic hospital utilizing Lean methodology – the process waste reduction component of LSS 39. Over 4,000 cases were reviewed from seven months of retrospective and seven months of prospective data. The study concluded that on-time first case starts increased from 57% (1,243) to 69% (1,595).
With appropriate utilization, LSS has been identified as an effective tool to reducing surgical cancellation within specific service lines and across larger systems. Additionally, LSS strategies may be successfully implemented to improve OR efficiency.
Integration of Mobile Health Technology
The presence of accessible mobile technology is a defining property of modern healthcare. In the United States, 90% of adults today own and utilize a smartphone 40. This leverageable aspect of the current healthcare landscape may offer a potential solution to the challenge of unexpected surgery cancellation. Health systems are responsible for numerous preparatory actions leading up to surgery. Some tasks, however, fall into the domain of patient responsibility. These tasks include arriving for surgery in a timely manner and adhering to preoperative instructions such as food and medication consumption. A study of 261 same-day surgery cancellations concluded that 17.6% (46) were a result of patient error, including failure to appear and failure to follow preoperative instructions 15. While these complications are perceived as the sole responsibility of the patient, system-level interventions may reduce the volume of these occurrences. Mobile technology provides a platform to assist patients in understanding surgical needs and reducing barriers to surgical care.
Applications for mobile smart devices have already been integrated into many service lines of care. Epic, an electronic medical record (EMR) system, offers the “My Chart” patient portal, which is accessible to 78% of patients in the United States 41. Research into similar mobile application technology for surgical preparation is ongoing. A study of spine surgery cases compared the compliance of mobile application users to a control group 42. The application provided patients with instruction reminders, checklists, and education. Of the 85 surgical patients utilizing the application, there were no surgical cancellations, and 100% compliance with preoperative instructions was achieved. In the control group, 5.6% (5) of the 89 surgeries were cancelled on the date of service. A similar mobile application was trialed among cataract surgery patients in one ophthalmology department 43. A total of 60 surgical patients were selected and randomly divided into control and intervention groups. Among non-application users, 6.7% (2) were cancelled on the date of service, while no cancellation occurred in the application user group. Additionally, the study noted that preoperative medication compliance more than doubled with utilization of the mobile application.
Mobile applications offer a potential avenue to improve patient compliance, however, inequities in access may present one barrier to this solution. While 90% of American adults own a smartphone, suburban residents are 17.8% more likely to have home internet services than rural residents and 11.6% more likely than urban residents 40. Utilization of short message service (SMS) texts mitigates the impact of this inequity. One evaluation of the technological and operational processes to create an SMS surgery reminder tool concluded that the software was “viable and easy to implement” 44. Multiple studies have identified the efficacy of such tools. One implementation of SMS reminders was trialed in prostate surgery patients 45. A control group of 473 patients was compared to an intervention group of 359 patients who received reminder texts in the two weeks leading to their procedure. The overall cancellation rate in the intervention group was 37.3% (160 vs 79) lower, and same-day cancellations were reduced by 86.8% (18 vs 2). A similar tool was studied in its impact to reduce cancellation for non-English speaking patients undergoing colonoscopies 46. Of the 1,299 patients included in the study, same-day cancellation was 52.2% (190 vs 58) higher among patients who did not receive SMS reminders.
Digitally accessible patient-centered education presents another pathway to reducing last-minute case cancellation. A survey to quantify “anxiety score” on the day of surgery was provided to patients undergoing thyroidectomy 47. Of the 36 patients provided with nurse-led online education, the mean anxiety score was 34. By comparison, the mean anxiety score was 59 within the group of 40 patients who did not receive nurse-led online education. In a separate study, a video-based educational series was trailed in the urology department of a pediatric hospital 48. Five months of pre-intervention and post-intervention data was collected. The same-day cancellation rate reduced from 7.47% (70 of 937) to 3.29% (43 of 1,306) in the post-intervention group. A similar video-based patient education initiative was evaluated in a study of 560 patients undergoing penile prosthetic surgery 49. In the control group, 37.6% (85) of cases were cancelled or rescheduled. This number was reduced to 13.2% (44) within the intervention cohort.
Mobile health technology is a growing field that is represented in various formats. Smartphone applications, SMS reminder services, and web-based patient education are all interventions that offer modern, accessible support to improving surgical attendance.
Discussion
The literature provides evidence-based support for the three proposed interventions to reduce last-minute surgical cancellations. Resources were selected based on their demonstrated impact and their ability to support viable interventions. Further analysis of these solutions is necessary to assess their real-world applicability. The Centers for Disease Control and Prevention propose five components of a best practice model for public health impact: effectiveness, reach, feasibility, transferability, and sustainability 50. This discussion provides a critical evaluation of each intervention using this framework of best practice.
Effectiveness
The effectiveness of an intervention is defined by its capacity to produce a desired outcome. The primary measurable outcome in this context is reduction in last-minute surgery cancellation. Resulting impacts of this outcome include improved patient health and financial benefit to health systems that deliver surgical care. Each of the three solutions examined in the literature review were found to provide varying degrees of effectiveness.
Resources pertaining to the integration of mobile health technology indicate that this intervention produces the greatest degree of effectiveness. Studies of the impact of this strategy reported 0% same-day cancellation rates in cohorts of patients who utilized a mobile health app to track surgical preparation 42, 43. Deployment of SMS reminders has reduced last-minute cancellation incidence by 86.8% and 52.2% in previous trials 45, 46. These studies document superior effectiveness than studies evaluating the optimization of preoperative services, although this intervention did produce positive outcomes as well. One integrated preoperative “One-Stop Shop” reduced same-day surgical cancellation by 70% 31. In contrast, less favorable outcome improvements have been reported, with post-intervention case cancellation decreases of as little as 2% 28.
Process improvement through LSS has exhibited notable success, however, in comparison to preoperative service optimization and mobile health technology, limited research is available regarding LSS’s direct impact on reducing case cancellation. Two studies draw clear conclusions on this topic, highlighting reductions in case cancellation by 74% and 42% 34, 36. Despite the success documented within these studies, the limited availability of research on this topic impacts the ability to accurately claim effectiveness of the solution.
Reach
The reach of an intervention refers to the scope at which it produces the intended outcome. Reach considers what populations are affected by the intervention as well as the scale of impact. The primary targets of the interventions are patients undergoing surgery and the financial environments of health systems. As the reach of an intervention is defined in part by its affected individuals, health equity is examined within this domain.
Preoperative service optimization supports a platform in which all patients are delivered the same level of care. The outcome of this is a solution to surgical cancellation that achieves the highest degree of reach. A foundational element within the design of this service is that standardization of services ensures that all patients undergoing surgery receive the same inputs. A distinct example of this is presented in the preoperative “One-Stop Shop” project 31.
Preoperative clinics such as this support patient outcomes, and the standardization of processes supports health equity. Additionally, this approach presents distinct evidence of financial return to health systems. LSS techniques yield a similar degree of reach by eliminating process waste and reducing variance. In statistics, a process achieving Six Sigma produces only 3.4 defects per 1 million events 33. High reliability associated with Six Sigma produces consistency of health outcomes. The Institute of Industrial and Systems Engineers notes that in health systems that appropriately utilized LSS, “they gained efficiency through more effective use of employees, leadership and management” 51.
The limited capacity of mobile health technology to deliver service universally reduces the intervention’s overall reach below that of the previous solutions. Within the United States, 1 in 10 adults do not own a smartphone capable of utilizing the proposed technology 40. Equitable access to services is also limited within this solution. Rural citizens are less likely to have access to internet at home, and adults above the age of 65 use smartphones significantly less than younger citizens, despite growing tech literacy across the board 40, 52.
Feasibility
A wide range of inputs are necessary to fully implement each of the three solutions in any level of healthcare facility. Perhaps the most significant of these inputs is capital. Both the cost of implementation and the cost of maintenance are essential considerations to the feasibility of an intervention. Consequently, one of the most prominent barriers to each solution is the potential inability to secure sufficient funding. Beyond capital, implementation of solutions would require stakeholder engagement, staffing, education and training, and data analysis.
Training for LSS programs can be achieved with minimal cost to health systems. Administrators and clinical leaders can obtain initial LSS certifications for less than $500 per individual, although official certification is not required for professionals to adopt LSS methodologies 53. Initiating LSS techniques requires minimal training costs to health systems, and numerous organizations already employ professionals with LSS training. Since 2005, the healthcare industry has adopted and continually developed the framework 54. The implementation of preoperative clinics is another low-cost solution to reducing surgical cancellations, although the up-front cost faces variance based on staffing and available resources. A nurse-led preoperative program within the ophthalmology department of an urban academic medical center cost just $35,970 annually, including the cost of implementation and training 22. By comparison, the national median salary of one full-time registered nurse is $93,600 55. Both interventions may be established with higher feasibility than mobile health technology, which is often associated with high costs. The approximate cost to design and implement a mobile healthcare application ranges from $30,000 to $250,000 based on the size of the partnering health organization 56. This cost burden greatly impacts the potential financial barrier to enactment, and consequently reduces the solution’s feasibility.
While preoperative services and mobile health technology may require the acquisition of new resources, LSS strictly focuses on improving task efficiency of existing systems. For this reason, process improvement through LSS is the most feasible solution to implement.
Sustainability
The implementation period of an intervention requires numerous inputs. The subsequent maintenance of an intervention requires consumption of resources over time. The feasibility of a solution is defined by its ability to continually achieve intended outcomes and the volume of resources required to maintain it.
The fundamental process utilized in LSS methodology is the Define, Measure, Analyze, Improve, Control (DMAIC) Cycle 57. Rather than a series of linear steps, DMAIC constitutes a repetitive process in which inputs and outcomes are continually examined. Following this cycle, health systems enable uninterrupted process improvement through LSS without producing entirely new resource demands. This element of the methodology makes it the most sustainable of the proposed interventions. Preoperative service optimization closely follows with its generally low maintenance costs. However, the intervention requires a greater degree of input commitment over time than LSS methodologies. With a maintenance cost of less than $40,000 annually, the initiative only requires workforce training to continually operate 22.
Both LSS and preoperative optimization provide more sustainable solutions to surgical cancellation than the integration of mobile health technology. Digital operating systems become outdated, hardware becomes obsolete, and mobile applications undergo routine updates. While the other two solutions are not immune to the cost of improvement, mobile health technology incurs the highest continual financial burden. Ohio Health, a not-for-profit organization based in Columbus, Ohio, paid $12 million for a single EHR system upgrade last year 58. Sustainability is one of the chief barriers to integrating mobile technology.
Transferability
A solution’s transferability is evaluated on the extent to which it can be successfully implemented in varying settings 50. In this context, transferable solutions are those that can be replicated across surgical specialties, organizational sizes, and clinical departments. Adaptability of an intervention is a key driver of overall transferability, as numerous variables may affect successful implementation.
Process improvement through LSS provides the highest degree of transferability by an appreciable margin. Before entering the healthcare landscape, LSS was utilized by leaders in the manufacturing industry to improve consistency and reduce waste 54. The methodology is now employed by health administrators across diverse service lines with reproducible success. In Cleveland Clinic, for example, the “Continuous Improvement Department” employs LSS strategies, which aided the program in reducing call center abandonment rate (639/day) by 30% 59. Mobile health technology provides comparable transferability to LSS, however, considerable barriers such as up-front cost reduce the applicability of mobile technology within lower revenue facilities. Rural community hospitals, for instance, may lack the necessary means to implement this solution. These facilities are already 9.4% less likely to possess certified EHR systems than large, urban hospitals 60. However, literature supports the solution’s transferability across procedural settings. Efficacy is concluded within studies occurring in prostate biopsy centers, colonoscopy clinics, spine surgery theaters, and ophthalmology departments. Similarly, preoperative clinics have been successfully integrated across multiple service lines. Studies identifying effective outcomes have been implemented in pediatric surgery, urological surgery, and multi-specialty departments. Further assessment of the intervention’s impact in varying settings of the surgical landscape is necessary to strengthen its overall transferability.
Recommendation
Surgical facilities account for a significant portion of the revenues and costs within the financial landscapes of many healthcare organizations 9. When last-minute, unplanned surgical cancellation occurs, OR time often goes unutilized. In these instances, health systems continue to incur the substantial overhead costs of OR operations without generating any corresponding revenue. In the health system of the United States, which performs 64 million completed surgeries annually, the incidence of same-day cancellation is roughly 10% 2, 20. Based on the best practice analysis of the available literature, it is recommended that healthcare organizations optimize their preoperative services through the implementation of a standardized preoperative clinic.
The effectiveness of these clinics has been concluded in a range of surgical settings, from independent ASCs to entire surgery departments of large academic hospitals. Studies pertaining to this strategy report reductions in last-minute surgical cancellation of around 50% 25, 31. Interventions associated with preoperative clinics have attained success with nurse-led programs, division-led programs, anesthesia-led programs, and interdisciplinary programs. The primary consistency within each of these interventions is that preoperative clinics developed and followed a standardized process. By screening each patient under the same guidelines, clinics produced impact of significant reach and delivered equitable healthcare services.
Several modalities of preoperative optimization exist, and various formats of preoperative clinics may suit the needs of one healthcare organization over another. Both the feasibility and sustainability of this approach have been demonstrated with the implementation of a nurse-led clinic that cost only $35,970 annually to operate and yielded a 61% return on investment 22. In large hospital settings with sufficient staffing, the nurse-led preoperative clinic is the recommended intervention due to its relatively low cost of implementation and maintenance.
Conclusion
Last-minute surgical cancellation is a considerable challenge for health administrators in the United States to address. Without sufficient notice, cancellations may result in unutilized OR time, which comes at a cost of $2,040 per hour to healthcare organizations 11. Additionally, same-day surgical cancellation has the potential to bear negative consequences on patient outcomes. A literature review prioritizing current, quantitative research was conducted to determine three evidence-based solutions to this health system challenge. Optimization of preoperative services, process improvement through Lean Six Sigma, and integration of mobile health technology were selected and subsequently evaluated through a model of best practices in public health impact. The analysis of best practice identified optimization of preoperative services as the ideal solution to reducing last-minute cancellation. This can be effectively achieved through the implementation of standardized, nurse-led preoperative clinics. Health systems may pursue this approach at a low cost without the requirement to obtain any new resources. Further research is needed to examine the direct financial impact of preoperative clinics, as well as the full extent of potential opportunities in preoperative optimization. Expanding the ability of these clinics to include financial navigation, coordination with ambulatory clinics, and social work may enhance their effectiveness. Incorporation of these non-clinical services will inherently inflate the cost of implementation, but may serve to maximize the benefit attained from preoperative programs.
References
1. Dobson GP. Trauma of major surgery: a global problem that is not going away. Int J Surg. 2020;81:47-54. doi:10.1016/j.ijsu.2020.07.017
2. Darrow JJ. Explaining the absence of surgical procedure regulation. Cornell J Law Public Policy. 2017;27(1):189-206. https://pubmed.ncbi.nlm.nih.gov/29239595/
3. McDermott KW, Liang L. Overview of major ambulatory surgeries performed in hospital-owned facilities, 2019. Agency for Healthcare Research and Quality. 2021. https://pubmed.ncbi.nlm.nih.gov/35107914/
4. McDermott KW, Liang L. Overview of operating room procedures during inpatient stays in U.S. hospitals, 2018. 2021. https://www.ncbi.nlm.nih.gov/books/NBK574416/
5. Dall T, Reynolds R, Chakrabarti R, et al. The complexities of physician supply and demand: projections from 2021 to 2036. Association of American Medical Colleges. 2024.
6. Bicket MC, Chua K-P, Lagisetty P, et al. Prevalence of surgery among individuals in the United States. Ann Surg Open. 2024;5(2):e421. doi:10.1097/as9.0000000000000421
7. Cubanski J, Neuman T. What to know about Medicare spending and financing. Kaiser Family Foundation. 2023. https://www.kff.org/medicare/issue-brief/what-to-know-about-medicare-spending-and-financing/
8. Kaye DR, Luckenbaugh AN, Oerline M, et al. Understanding the costs associated with surgical care delivery in the Medicare population. Ann Surg. 2020;271(1):23-28. doi:10.1097/sla.0000000000003165
9. Rothstein DH, Raval MV. Operating room efficiency. Semin Pediatr Surg. 2018;27(2):79-85. doi:10.1053/j.sempedsurg.2018.02.004
10. Hawkins M. 2019 Physician Inpatient/Outpatient Revenue Survey. AMN Healthcare. 2019.
11. Childers CP, Maggard-Gibbons M. Understanding costs of care in the operating room. JAMA Surg. 2018;153(4):e176233. doi:10.1001/jamasurg.2017.6233
12. Smith T, Evans J, Moriel K, et al. Cost of OR time is $46.04 per minute. J Orthop Business. 2022;2(4):10-13. doi:10.55576/job.v2i4.23
13. Elliott‐Dawe C, Chen J, Stucky CH, Zadinsky JK. Retrospective analysis of associated costs and sources of variability in OR utilization across weekdays. AORN J. 2024;120(1). doi:10.1002/aorn.14164
14. Gruson KI, Lo Y, Volaski H, Sharfman Z, Shah P. Incidence and risk factors for patient-related short-term cancellation of elective arthroscopic surgery: a case-matched study. JAAOS Glob Res Rev. 2022;6(4). doi:10.5435/jaaosglobal-d-22-00034
15. Kaddoum R, Fadlallah R, Hitti E, El-Jardali F, El Eid G. Causes of cancellations on the day of surgery at a tertiary teaching hospital. BMC Health Serv Res. 2016;16(1). doi:10.1186/s12913-016-1475-6
16. Koh WX, Phelan R, Hopman WM, Engen D. Cancellation of elective surgery: rates, reasons and effect on patient satisfaction. Can J Surg. 2021;64(2):E155-E161. doi:10.1503/cjs.008119
17. Turcotte JJ, Brennan JC, Kidd G, Zaidi SN. Predictors of same day cancellation of elective surgery. J Perioper Pract. 2024;34(6):178-186. doi:10.1177/17504589231189349
18. Smith BB, Smith MM, Hyder JA, et al. Same-day cancellation in ambulatory surgery: a retrospective review at a large academic tertiary referral center. J Ambul Care Manage. 2018;41(2):118-127. doi:10.1097/jac.0000000000000226
19. Viftrup A, Laustsen S, Pahle ML, Dreyer P, Nikolajsen L. Patient-reported harm following cancellation of planned surgery at a Danish university hospital: a cross-sectional study. BMJ Open. 2024;14(11):e082807. doi:10.1136/bmjopen-2023-082807
20. Schuster M, Neumann C, Neumann K, et al. The effect of hospital size and surgical service on case cancellation in elective surgery. Anesth Analg. 2011;113(3):578-585. doi:10.1213/ane.0b013e318222be4d
21. Stafinski T, Nagase FNI, Brindle ME, et al. Reducing wait times to surgery—an international review. J Hosp Manag Health Policy. 2022;6:29. doi:10.21037/jhmhp-21-96
22. Kuelz A. Strategic policy development to reduce same-day cancellations: a nurse-led preoperative approach. University of San Diego. 2025. doi:10.22371/07.2025.026
23. Cumberland L. Preparing for surgery? What you need to know. Mayo Clinic. 2022. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/preparing-for-surgery-what-you-need-to-know
24. Berlin NL, Yost ML, Cheng B, et al. Patterns and determinants of low-value preoperative testing in Michigan. JAMA Intern Med. 2021;181(8):1115. doi:10.1001/jamainternmed.2021.1653
25. Wolgemuth E, Glackin J, Linquist AB, et al. Implementation of a preanesthetic telehealth visit to reduce day-of-surgery cancellations. J PeriAnesth Nurs. 2025;40(2):265-269. doi:10.1016/j.jopan.2024.05.022
26. Sato M, Ida M, Naito Y, Kawaguchi M. The incidence and reasons for canceled surgical cases in an academic medical center: a retrospective analysis before and after the development of a preoperative anesthesia clinic. J Anesth. 2020;34(6):892-897. doi:10.1007/s00540-020-02841-4
27. Vig S, Gabriel RA, Schmidt U. Care center by an attending anesthesiologist is associated with a reduction in day-of-surgery cancellations. Physician Leadersh. 2020. https://www.physicianleaders.org/articles/management-preoperative-care-center-attending-anesthesiologist-is-associated-reduction-day-surgery-cancellations
28. Sweetman S, Sharkey AR, Thomas K, Dhesi J. Reduction of last-minute cancellations in elective urology surgery: a quality improvement study. Int J Surg. 2020;74:29-33. doi:10.1016/j.ijsu.2019.12.011
29. Spazzapan M, Javier P, Abu-Ghanem Y, et al. Reducing last-minute cancellations of elective urological surgery—effectiveness of specialist nurse preoperative assessment. Int J Qual Health Care. 2023;35(1). doi:10.1093/intqhc/mzad008
30. Lee CM, Rodgers C, Oh AK, Muckler VC. Reducing surgery cancellations at a pediatric ambulatory surgery center. AORN J. 2017;105(4):384-391. doi:10.1016/j.aorn.2017.01.011
31. Benedictos A. Improving patient safety for surgical clearance: a preop one stop shop. University of San Francisco. 2023. https://repository.usfca.edu/dnp/331/
32. Umeno Y, Ishikawa S, Kudoh O, Hayashida M. Effects of the multidisciplinary preoperative clinic on the incidence of elective surgery cancellation. J Med Syst. 2022;46(12). doi:10.1007/s10916-022-01883-3
33. Harry MJ. Six sigma: a breakthrough strategy for profitability. Qual Prog. 1998;31(5). https://asq.org/quality-progress/articles/six-sigma-a-breakthrough-strategy-for-profitability?id=bd6baa689df842a3905d068dd52d2120&srsltid=AfmBOooiyyln2FTUo8Vblk2P11rAheRol_pqrtFFdLndeYX966opTNA2
34. Schretlen S, Hoefsmit P, Kats S, et al. Reducing surgical cancellations: a successful application of Lean Six Sigma in healthcare. BMJ Open Qual. 2021;10(3):e001342. doi:10.1136/bmjoq-2021-001342
35. Daly A, Wolfe N, Teeling SP, Ward M, McNamara M. Redesigning the process for scheduling elective orthopaedic surgery: a combined Lean Six Sigma and person-centred approach. Int J Environ Res Public Health. 2021;18(22):11946. doi:10.3390/ijerph182211946
36. Zhu L-F, Qian W-Y, Zhou G, et al. Applying Lean Six Sigma to reduce the incidence of unplanned surgery cancellation at a large comprehensive tertiary hospital in China. J Health Care Organ Provision Financ. 2020;57. doi:10.1177/0046958020953997
37. Hicks KB, Glaser K, Scott C, Sparks D, McHenry CR. Enumerating the causes and burden of first case operating room delays. Am J Surg. 2020;219(3):486-489. doi:10.1016/j.amjsurg.2019.09.016
38. Mitchell CV, Anderson AR, Romito K, Abadie WM, Phillips AK. Employing lean six sigma strategies to improve operating room first case on-time starts: a case report. Perioper Care Oper Room Manag. 2025;38:100473. doi:10.1016/j.pcorm.2025.100473
39. Deldar R, Soleimani T, Harmon C, et al. Improving first case start times using Lean in an academic medical center. Am J Surg. 2017;213(6):991-995. doi:10.1016/j.amjsurg.2016.08.025
40. Gelles-Watnick R. Americans’ use of mobile technology and home broadband. Pew Research Center. 2024. https://www.pewresearch.org/internet/2024/01/31/americans-use-of-mobile-technology-and-home-broadband/
41. Johnson Memorial Health Services. EPIC EMR Updates. 2022. https://jmhsmn.org/epic-emr-updates/
42. Stewart JJ, Fayed I, Henault S, Kalantar B, Voyadzis J-M. Use of a smartphone application for spine surgery improves patient adherence with preoperative instructions and decreases last-minute surgery cancellations. Cureus. 2019. doi:10.7759/cureus.4192
43. Sharp. Mobile app (Sharp Health Companion) designed to help patients prepare & recover from cataract surgery. American Board of Ophthalmology. 2020.
44. Souza DAG, Araújo-Filho I, Cabral ELDS, et al. Surgery remember@: an innovation to reduce surgical cancellations. Rev Col Bras Cir. 2021;48. doi:10.1590/0100-6991e-20213206
45. Balakrishnan AS, Nguyen HG, Shinohara K, Au Yeung R, Carroll PR, Odisho AY. A mobile health intervention for prostate biopsy patients reduces appointment cancellations: cohort study. J Med Internet Res. 2019;21(6):e14094. doi:10.2196/14094
46. Zapata MC, Ha JB, Hernandez-Barco YG, Richter JM. Using a customized SMS program to promote colonoscopy adherence and support bowel cleanliness for Spanish-speaking patients. J Health Care Poor Underserved. 2022;33(2):1069-1082. doi:10.1353/hpu.2022.0081
47. Altinbas BC, Gürsoy A. Nurse‐led web‐based patient education reduces anxiety in thyroidectomy patients: a randomized controlled study. Int J Nurs Pract. 2023;29(3). doi:10.1111/ijn.13131
48. Kim E, Canadas K, Geistkemper C, et al. MP76-15 patient focused education via smartphone: is it effective in decreasing same day surgery cancellation rate? J Urol. 2018;199(4S). doi:10.1016/j.juro.2018.02.2583
49. Ballon-Landa E, Clavijo R, Gross M, et al. A novel video-based patient education program to reduce penile prosthetic surgery cancellations. Am J Mens Health. 2019;13(6):155798831989356. doi:10.1177/1557988319893568
50. Spencer LM, Schooley MW, Anderson LA, et al. Seeking best practices: a conceptual framework for planning and improving evidence-based practices. Prev Chronic Dis. 2013;10. doi:10.5888/pcd10.130186
51. Galli BJ. The economics of lean Six Sigma in healthcare. Institute of Industrial & Systems Engineers. 2017. https://www.iise.org/details.aspx?pageid=43500&id=45815
52. Faverio M. Share of those 65 and older who are tech users has grown in the past decade. Pew Research Center. 2022. https://www.pewresearch.org/short-reads/2022/01/13/share-of-those-65-and-older-who-are-tech-users-has-grown-in-the-past-decade/
53. American Society for Quality. Lean Six Sigma Training. 2025. https://asq.org/training/lean-six-sigma?srsltid=AfmBOorquBemrpauOQnAJonlliIEGAcH3sdqi6KBDu-eHTBm_zQLOGR
54. Rathi R, Vakharia A, Shadab M. Lean six sigma in the healthcare sector: a systematic literature review. Mater Today Proc. 2022;50:773-781. doi:10.1016/j.matpr.2021.05.534
55. U.S. Bureau of Labor Statistics. Registered nurses. 2025. https://www.bls.gov/ooh/healthcare/registered-nurses.htm
56. Bhargava N. A complete breakdown of healthcare app development cost in 2025. Akra Softwares. 2025. https://www.arkasoftwares.com/blog/a-complete-breakdown-of-healthcare-app-development-cost-in-2025/
57. Monday LM. Define, Measure, Analyze, Improve, Control (DMAIC) methodology as a roadmap in quality improvement. Glob J Qual Saf Healthc. 2022;5(2):44-46. doi:10.36401/jqsh-22-x2
58. Diaz N. OhioHealth hospital spends $12M on EHR upgrade. Becker's Health IT. 2024. https://www.beckershospitalreview.com/healthcare-information-technology/ehrs/ohiohealth-hospital-spends-12m-on-ehr-upgrade/
59. Zhao Y. Six Sigma in the Cleveland Clinic call center. Scientific Open Access Publishing. 2024. https://www.researchgate.net/publication/386061816_Six_Sigma_in_the_Cleveland_Clinic_Call_Center/link/674192e96dedd318c895d8cd/download?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0aW9uIn19
60. Office of the National Coordinator for Health IT. Percent of hospitals, by type, that possess certified health IT. 2018. https://www.healthit.gov/data/quickstats/percent-hospitals-type-possess-certified-health-it