The Evolution and Transformation of Partners in Health: From Non-Governmental Organization to Global Health Relief and Development
Krupa Patel, DHA, MBEMH, MHA, MGH, Oklahoma State University Center for Health Sciences
Anil Kaul, MD, DDS, MPH, Oklahoma State University Center for Health Sciences
Corresponding Author:
Krupa Patel, DHA, MBEMH, MHA, MGH
Oklahoma State University Center for Health Sciences
1111 W. 17 Street
Tulsa, OK 74107
Funding Statement:
No external funding was received for this study.
Conflict of Interest Disclosure:
The authors declare no financial or non-financial conflicts of interest.
Data Availability Statement
No primary data was generated for this study. All data used are from publicly available sources cited in the manuscript.
Author Contributions
The authors conceptualized the study, conducted the literature review and analysis, drafted the manuscript, and approved the final version.
Acknowledgements
The authors acknowledge the contributions of researchers and practitioners whose work informed this study.
Abstract
Background
Non-governmental organizations (NGOs) have increasingly played an important role in addressing global health inequities. Partners In Health (PIH), founded in 1983, illustrates the evolution of NGOs from localized charitable initiatives into global health relief and development institutions.
Objectives
This paper examines the transformation of Partners in Health from a community clinic in Cange, Haiti, into a multinational organization working with ministries of health across several regions.
Summary of Model
This manuscript presents a narrative review and conceptual analysis of the evolution of Partners in Health and its role in advancing equity‑focused global health systems. Central to PIH’s work is the accompaniment model, emphasizing long‑term partnerships with patients and communities while addressing social determinants of health.
Conclusion
PIH represents a shift from charity-based NGO models toward equity‑driven health systems strengthening.
Keywords: Partners In Health, Non-Governmental Organizations (NGOs), Global Health, Health Equity, Health Systems Strengthening, Social Determinants of Health
Introduction
This paper argues that Partners in Health (PIH) represents a paradigm shift from charity-based NGO models toward equity-driven health systems strengthening built on long-term community partnerships and sustained collaboration with national health systems.
The origins of non-governmental organizations (NGOs) date back to the 1800s, when religious and charitable groups formed local organizations to address poverty in urban communities.¹ Some of these organizations were war-related and were established to provide medical care, assist orphaned children, and deliver supplies to areas affected by war.¹ Even though many early organizations operated without formal names, the first officially documented national NGO is often cited as the Anti-Slavery Society, founded in 1839 to promote the immediate abolition of slavery in the United States.² In 1945, when the United Nations (UN) was created, the term “non-governmental organization” first took on its modern, bureaucratic meaning when it appeared in Chapter 10, Article 71 of the United Nations Charter.³ The Charter broadly defined NGOs as organizations that are independent of government administration, non-profit in nature, and able to include specialized private agencies.³
Background: Founding and Expansion of Partners in Health
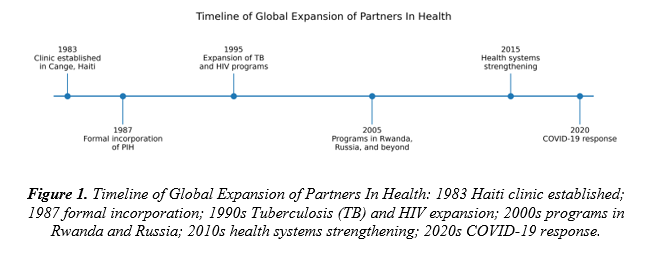
Partners in Health, an NGO based in Boston, was founded more than thirty years ago, in 1983.⁴ Partners in Health was formed to support a small Haitian village called Cange, located in Haiti’s Central Plateau.⁴ The organization’s founders, Paul Farmer and Ophelia Dahl, opened a small community clinic in hopes of alleviating the village’s healthcare burden.⁶ In 1987, Farmer and Dahl expanded their efforts by allowing Thomas J. White, Jim Yong Kim, and Todd McCormack to join their clinic, officially creating Partners in Health, to support the work of providing free healthcare to all patients across Haiti.⁴ From Haiti’s Central Plateau, Partners in Health expanded their mission and commitment to Peru, Russia, Africa, Mexico, and the Navajo Nation within the United States.⁵ Over the years, the organization has evolved, but its commitment to solidarity and advocacy for disadvantaged populations has remained constant.⁷ Today, Partners In Health is a democratic health organization. Although it was originally inspired by liberation theology, it now operates independently of ideological affiliations and works closely with health ministries to improve access to care over the long term.⁴,⁹
While the work began in 1983, Partners in Health was formally incorporated in 1987 when Thomas J. White, Jim Yong Kim, and Todd McCormack joined the founders. This distinction clarifies the early development timeline.
Mission and Comprehensive Model of Care
Through its evolution, Partners In Health has remained committed to its mission of promoting health equity by delivering high-quality healthcare services to underserved populations worldwide.⁷ As an organization, their goal has always been to alleviate pain and suffering through a comprehensive approach that enables care by encompassing essentials like food, transportation, housing, and other vital aspects of recovery.⁸ The organization seeks to extend modern medical advances to populations historically affected by structural inequalities while affirming that all lives hold equal value.¹⁰ Through their mission, Partners In Health has strived to offer services in impoverished regions of developing nations.⁷ They have established hospitals and healthcare facilities where they have set new standards for how healthcare professionals are trained to offer medical treatments, from wellness check-ups to cancer care.¹³ Additionally, they address challenges like contaminated water and food scarcity to promote better health outcomes for the underprivileged and encourage healthier dietary practices among underserved populations.¹²
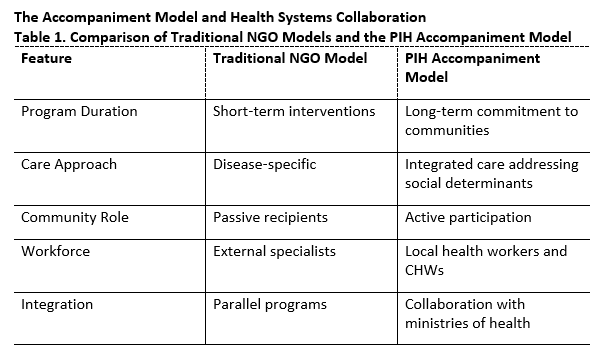
To advance global health relief and development, Partners In Health has expanded its operations across numerous countries to address similar health challenges affecting underserved populations.¹⁰ Their growth has been accompanied by the establishment of their healthcare model called "accompaniment," which focuses on making a long-term commitment to communities by addressing both their health needs and the underlying social factors affecting health.⁹ Through their work, Partners in Health has forged enduring connections with sister organizations situated in areas aiming to extend the advancements of medical science to those facing the greatest hardships.¹⁰ By leveraging the expertise of academic institutions and drawing inspiration from the resilience of underprivileged and ailing communities worldwide, Partners in Health works in tandem with local health ministries to devise and execute holistic health programs that strengthen healthcare systems.¹³ By embracing the "accompaniment" healthcare model, Partners in Health has fostered private partnerships which have become crucial for upholding healthcare services and infrastructure sustainability within their organization.⁹
Global Health Relief and Development Work
Evidence from multiple PIH-supported programs demonstrates measurable clinical outcomes. In Haiti, community-based tuberculosis treatment programs supported by PIH achieved cure rates exceeding 80-90%, significantly higher than many comparable low-resource settings during the same period. In Rwanda, collaboration with the Ministry of Health contributed to major improvements in maternal and child health services, including increased facility-based deliveries and expanded Human Immunodeficiency Virus (HIV) treatment coverage. These measurable outcomes illustrate how the accompaniment model can translate into quantifiable improvements in population health.
From global health relief to global health development, Partners In Health has contributed to fighting various global health crises such as Human Immunodeficiency Virus / Acquired Immunodeficiency Syndrome (HIV/AIDS), tuberculosis, cholera outbreaks, and the Ebola virus outbreak in West Africa.¹⁰ The organization has contributed to the transformation of global health relief and development by addressing crises through comprehensive strategies that reduce immediate impacts while strengthening long-term societal resilience.¹² Partners In Health’s role in global health relief and development has always been multifaceted, where it has aimed to assist those in immediate crises, worked to ameliorate major health threats, and have continued to provide public healthcare for the underprivileged and marginalized populations.¹¹
Workforce Development and Task Shifting
Furthermore, Partners in Health has acknowledged the significance of enhancing healthcare systems in areas where resources are limited by focusing on developing infrastructure, enhancing skills, and providing access to medications and technologies.¹³ By training local healthcare workers and improving the conditions of healthcare facilities, Partners In Health has contributed to more durable improvements in health outcomes by focusing on regions where resource-limited healthcare systems grapple with shortages of trained staff, frontline workers, and adequate infrastructure.¹³ To continue their response towards global health relief and development, they have focused on task shifting, trying to deliver clinical services where fewer highly skilled providers handle more complex tasks resulting in nurses and other healthcare professionals taking on roles typically reserved for high-level personnel.¹⁴
Advocacy, Policy, and Research
Both domestically and globally, Partners In Health has been involved in advocacy to shape public health policy.¹⁵ Other than providing healthcare to the underserved and underprivileged, they also advocate for policies to address the social determinants of health and poverty, campaigning for cancellation of the healthcare debts of citizens in underserved countries, free access to lifesaving drugs, and universal health insurance.¹⁵ By advocating for the change of policies and national laws, the organization helps make a positive impact that will have a lasting effect on the underlying structural causes of poor health.¹⁸ Moreover, like most hospitals and healthcare centers, Partners in Health also invests in conducting research that could lead to groundbreaking development in new and non-invasive medical treatments.¹⁶ Partners in Health are devoted to evaluation of the efficacy of their organization and they frequently collaborate with other organizations, academic institutions, and governments to forge cheaper, more effective methods of delivering care to the sickest and most vulnerable.¹³ By working with these organizations and institutions, Partners in Health leverages its resources and expertise to create a positive change by delivering healthcare directly where it is needed.¹⁶ The approach employed by Partners in Health as a role model has served as a model for effective and compassionate healthcare interventions worldwide.¹⁸
Ongoing Commitment to Social Justice and Health Equity
Nevertheless, despite its ever-broadening reach, Partners in Health’s evolution and transformation has not relinquished its original commitment to social justice and health equity, nor has it abandoned the accompaniment model that guides its medical practice.⁷ Partners in Health has remained faithful to its founding commitment of social justice and equitable healthcare delivery.⁷ The accompaniment model that frames its daily medical practice rests not only on medical care but also on the centrality of community empowerment and the importance of local leadership and communities taking control of their own health destinies.⁹ Partners in Health collaborates with international civil and nongovernmental organizations, governmental agencies, and local community leaders in ways that aim to foster and build an environment of trust and social capital.¹⁰ This ground-up healthcare approach has been successful and death rates that once defined entire communities are long gone.¹³
Integrated Development and Global Health Equity Advocacy
Additionally, over time, Partners in Health’s concerted social and economic integrated development approach has highlighted their efforts to address environmental, economic, and social determinants of poverty alongside the direct provision of care.¹⁸ They have introduced educational programs, vocational training initiatives, microfinance projects, and agricultural assistance to cooperatives.¹⁰ These endeavors are designed to complement the growing number of individuals who must navigate their lives amidst infectious diseases and economic challenges.¹⁸ Moreover, Partners in Health’s efforts have expanded beyond its initial focus on direct care provision. After successful projects in Rwanda, Tanzania, and Haiti, Partners in Health has invested significant energy in addressing global health inequities and advocating for health equity as a fundamental human right.¹⁸ Rigorous research, advocacy, and alliances with aligned groups have ensured that governments and institutions have been held accountable for ensuring universal health access, fair trade for life-saving drugs, and challenging discriminatory policies that perpetuate health inequities.¹⁸ These ongoing transformations underscore Partners in Health's evolution from a small non-profit organization in Boston to a more global entity advocating for direct medical care.¹⁰ It has grown into a major health relief and development organization, championing social justice, solidarity, and equity.⁷ Partners in Health’s local and international efforts in community engagement, innovation, and health equity advocacy serve as a commendable model of health ecumenicalism and dedicated service for humanity.¹⁸ In the face of obstacles that pose risks to community wellbeing, Partners in Health has served as a source of optimism. With health disparities growing, Partners in Health's unwavering dedication to improving health and fostering fairness stands out as an influence in our evolving society.⁷
Partners in Health During the COVID-19 Pandemic
During the Coronavirus Disease 2019 (COVID-19) pandemic, PIH supported testing infrastructure, clinical care delivery, and community outreach in multiple countries and U.S. settings. In Massachusetts, PIH partnered with state and local health authorities to support large-scale contact tracing initiatives and community health worker (CHW) outreach in vulnerable communities. Internationally, PIH assisted ministries of health in strengthening laboratory capacity, infection prevention protocols, and clinical training for healthcare workers. These activities helped expand testing capacity, improve case identification, and strengthen public health response capabilities in underserved settings.
Critical Reflections and Limitations
Despite its successes, the scalability and sustainability of the accompaniment model remain subjects of scholarly discussion. Implementing such an intensive model of care requires long-term financial commitments, strong governmental partnerships, and sustained workforce investment. Critics have noted that the model’s reliance on extensive community engagement and integrated social support services may present challenges when applied at national scale, particularly in countries with limited health financing. Additionally, partnerships with ministries of health can introduce administrative and political complexities that influence program implementation. Nevertheless, supporters argue that PIH’s approach demonstrates that equity-driven health system strengthening can produce meaningful health outcomes when combined with sustained investment, community engagement, and policy advocacy.
Compared with other major global health organizations, PIH's operational model emphasizes long-term partnership and health system strengthening. Organizations such as Medecins Sans Frontieres (MSF) primarily focus on rapid emergency medical response in conflict zones and humanitarian crises, while BRAC has historically emphasized large-scale development programming and poverty alleviation. In contrast, PIH integrates clinical care delivery with structural interventions such as community health worker programs, infrastructure development, and collaboration with national ministries of health to build durable health systems in resource-limited settings.
Conclusion
In conclusion, Partners in Health has gone through a transformation, from its beginnings as a small NGO in Boston to becoming a prominent global player in the realms of health and development.⁴ Initially established as a clinic in Haiti to highlight principles of justice and human compassion, it has now evolved into an expansive relief organization operating across various nations.¹⁰ The organization has shifted its focus from charitable endeavors to becoming an advocate for the underprivileged, carrying forward the spirit of a movement and demonstrating unwavering support.⁷ Its comprehensive approach, which incorporates education, job training, and preventive healthcare, extends beyond traditional philanthropy toward long-term health system strengthening.¹⁸ In the face of challenges brought about by the COVID-19 crisis, Partners in Health remained resolute to testing, treating, and researching the virus while driving advocacy efforts, policy reforms, and research at scale.¹⁹ By addressing the multifaceted factors that influence health outcomes, Partners in Health continues its mission “to ease suffering by providing a comprehensive model of care” while upholding its core value of helping people by offering the key components of healing, thereby exemplifying its pivotal role in global health relief and development.⁷
References
1. Odigie-Emmanuel, O. L., Blessing, N., Prince, W. C., Frank, R. F., Enyinda, B. O., Chima, A. G., & Chidiadi, Q. (2022). International institutions and non-governmental organization: Understanding their nature and functions in international law. Journal of Public and Private Law, 12.
2. Welch, C. E., Jr. (2008). Defining contemporary forms of slavery: Updating a venerable NGO (Buffalo Legal Studies Research Paper No. 2008-002). University at Buffalo, SUNY.
3. Jedele, C. (2020). Domestic restrictions on non-governmental organizations and potential protections through legal personality: Time for a change? Chicago Journal of International Law, 21(1). https://cjil.uchicago.edu/print-archive/domestic-restrictions-non-governmental-organizations-and-potential-protections
4. Block, J. W., Lysaught, M. T., & Martins, A. A. (Eds.). (2023). A prophet to the peoples: Paul Farmer’s witness and theological ethics (Global theological ethics). Pickwick Publications.
5. Partners In Health. (2021). Digital annual report 2021. https://www.pih.org/annual-report-2021/
6. Academy of Achievement. (2022). Paul Farmer, M.D. https://achievement.org/achiever/paul-farmer/
7. Partners In Health. (2019). Brand handbook. https://www.pih.org/sites/default/files/2019-11/Brand%20Handbook.pdf
8. Partners In Health. (2025). Mission. https://www.pih.org/our-mission/
9. Partners In Health. (2025). Building strong health systems. https://www.pih.org/our-approach
10. Farmer, P. (2010). Partner to the poor: A Paul Farmer reader (H. Saussy, Ed.). University of California Press. https://doi.org/10.1525/9780520945630
11. Kallon, L. H., Raven, J., Wurie, H. R., & Mansour, W. (2023). From policy to practice: A qualitative study exploring the role of community health workers during the COVID-19 response in Sierra Leone. BMC Health Services Research, 23(1), 1228. https://doi.org/10.1186/s12913-023-10272-6
12. Commission on a Global Health Risk Framework for the Future, & National Academy of Medicine. (2016). The neglected dimension of global security: A framework to counter infectious disease crises. National Academies Press. https://doi.org/10.17226/21891
13. National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Global Health; Committee on the Evaluation of Strengthening Human Resources for Health Capacity in the Republic of Rwanda Under the President’s Emergency Plan for AIDS Relief (PEPFAR). (2020). Evaluation of PEPFAR's contribution (2012–2017) to Rwanda's human resources for health program. National Academies Press. https://doi.org/10.17226/25687
14. Partners In Health. (2008). Task shifting. https://www.pih.org/article/task-shifting
15. Karan, A. (2016, July). Building ethical global health care systems. AMA Journal of Ethics, 18(7), 661. https://journalofethics.ama-assn.org/sites/joedb/files/2025-06/joe-1607.pdf
16. Partners In Health. (2025). Research. https://www.pih.org/programs/research
17. Behforouz, H. (2009). Accompaniment could be the key to reforming and transforming health care. Partners In Health. https://www.pih.org/article/accompaniment-could-be-the-key-to-reforming
18. Bukhman, G., Mocumbi, A. O., Atun, R., Becker, A. E., Bhutta, Z., Binagwaho, A., Clinton, C., Coates, M. M., Dain, K., Ezzati, M., Gottlieb, G., Gupta, I., Gupta, N., Hyder, A. A., Jain, Y., Kruk, M. E., Makani, J., Marx, A., Miranda, J. J., Norheim, O. F., Nugent, R., Roy, N., Stefan, C., Wallis, L., & Mayosi, B. (2020). The Lancet NCDI Poverty Commission: Bridging a gap in universal health coverage for the poorest billion. The Lancet, 396(10256), 991–1044. https://doi.org/10.1016/S0140-6736(20)31907-3
19. Partners In Health. (2025). Emergency response. https://www.pih.org/programs/emergency-response
20. Partners In Health. (2025). Home. https://www.pih.org/