Knowledge and Practice Regarding Occupational Hazards among Staff Nurses: A Cross Sectional Study from Nepal
Narendra TIMALSINA, PhD, MHA., Nepal Mediciti Hospital, Department of Quality & Patient Safety., Bhaisepati 18, Lalitpur 44700, Nepal
Sujita SENCHURY, BSN, RN., IMCU, Boston Medical Center.
Boston, MA 02118, USA
Corresponding email: narendratimalsina@gmail.com,
senchury.sujen@gmail.com,
ABSTRACT
Background: Nurses constitute the largest segment of the healthcare workforce and are frequently exposed to occupational hazards during patient care and clinical procedures. Strengthening their knowledge and practice is essential to reducing risk and improving workplace safety.
Objectives: This study assessed nurses’ knowledge and practices related to occupational hazards, examined differences across demographic categories, evaluated the association between knowledge and practice, and identified measures to improve compliance with occupational safety standards.
Methods: A descriptive cross sectional design was used. Data were collected from staff nurses using a pretested structured questionnaire. Descriptive statistics summarized knowledge and practice scores. Chi square tests examined differences in knowledge and practice across demographic variables, and Karl Pearson’s correlation coefficient assessed the relationship between knowledge and practice.
Results: The mean knowledge score was 18.38 (SD = 1.28). Chi square analysis showed no statistically significant differences in knowledge across demographic categories (χ² = 2.1854, p = 0.1393). The mean practice score was 15.68 (SD = 2.95), with no significant demographic differences (χ² = 0.1319, p = 0.7165). A positive, though weak, correlation was found between knowledge and practice (r = 0.0645, p = 0.7860), indicating that higher knowledge was modestly associated with better practice.
Conclusion: Although nurses demonstrated generally adequate knowledge and practice regarding occupational hazards, the weak correlation suggests gaps in translating knowledge into consistent practice. Regular training, continuous supervision, and structured learning packages on occupational safety may enhance compliance and strengthen safe clinical performance.
Key words: knowledge and practice, Occupational hazards, Universal precautions, hospital acquired infections, Healthcare compliance, Needle stick injury
INTRODUCTION
Healthcare environments expose workers—particularly nurses—to a wide range of occupational hazards, including physical, chemical, biological, and psychosocial risks. The extent of exposure and the effectiveness of preventive practices vary globally, influenced by differences in healthcare systems, training, and institutional safety cultures.
Studies from diverse regions highlight persistent gaps in occupational safety. Razei et al.1 reported significant safety concerns among pediatric nurses in Tehran, while Ashok2 identified occupational challenges among female healthcare workers in India. In Africa, Mossburg et al.3 documented widespread exposure to occupational injuries, compounded by limited access to post exposure prophylaxis, as also noted by Adinan et al.4 in Tanzania. Similar gaps in knowledge and safety practices have been reported in Nigeria (Amosu et al.5), Palestine (Al Khatib et al.6), and India (Senthil et al.7).
Recent studies emphasize the importance of early training and awareness. Amare et al.8 found that nursing students frequently encounter occupational hazards during clinical practice, while Alsabaani et al.9 highlighted inadequate knowledge of needle stick injury prevention among healthcare workers. Awareness of radiation hazards also remains limited, as shown by Khamtuikrua and Suksompong10.
Given these global findings, this study examines the knowledge and practices of staff nurses regarding occupational hazards in a tertiary hospital in Nepal. The goal is to identify gaps and propose targeted interventions to strengthen occupational safety.
OBJECTIVES
• To assess the level of knowledge and practice of nurses regarding occupational hazards.
• To determine the correlation between knowledge and practice.
• To identify measures to improve compliance with occupational hazard control at the Hospital.
MATERIALS AND METHODS
The study was conducted in a 272-bed tertiary hospital in Nepal over three months from June to August 2022. A total of 150 nurses participated in the study. Formal permission was obtained from the institutional review committee, and consent was taken from all participants. The research adopted a descriptive cross-sectional approach, collecting information via a pretested structured questionnaire.
The inclusion criteria targeted registered staff nurses employed at Hospital who were willing to participate. This ensured that the participant pool was both relevant and motivated. Conversely, the exclusion criteria eliminated certain groups: nurses who did not wish to participate, nurses with managerial responsibilities, and nurses on leave during data collection. This careful delineation ensured a focused and representative sample for the research.
Based on the study’s objectives and hypotheses, data analysis was performed using inferential statistics. Knowledge and practice scores were converted into categorical variables to facilitate Chi square analysis. The mean score for each domain served as the threshold. Participants scoring at or below the mean were categorized as having low knowledge/practice, while those scoring above the mean were categorized as having high knowledge/practice. This approach is commonly used in cross sectional studies where no established cut off values exist.
RESULTS
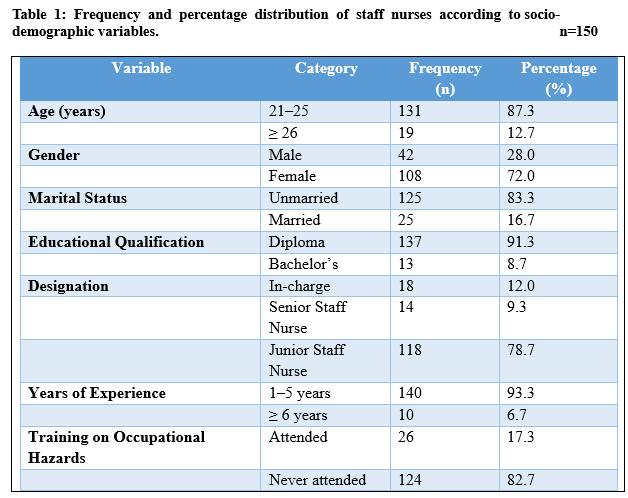
Data presented in table 1 indicate that, among the 150 nurses surveyed, every respondent completed the questionnaire, achieving a 100% response rate. A substantial majority of the staff nurses, 131 (87.33%), were aged between 21 and 25 years, with the remaining 19 (12.67%) being 26 years or older. Gender distribution revealed that most of the staff nurses were female, accounting for 108 (72%), while 42 (28%) were male.
In terms of marital status, 125 (83.33%) of the nurses were unmarried, whereas 25 (16.67%) were married. Educational qualifications showed that the vast majority, 137 (91.33%), had obtained a Diploma in General Nursing, while a smaller group of 13 (8.67%) had earned Bachelor’s degrees. Regarding job roles, 18 (12%) of the nurses held in-charge positions, 14 (9.33%) were senior staff nurses, and the majority, 118 (78.67%), were junior staff nurses. Experience levels varied, with 140 (93.33%) having 1-5 years of experience since obtaining their basic nursing qualification, and only 10 (6.67%) having more than 6 years of experience.
Additionally, the data highlighted that the majority of nurses, 124 (82.67%), had never undergone any in-service education or training in occupational hazards control, while 26 (17.33%) had attended such training programs. This emphasizes the need for increased training and awareness among staff nurses to ensure better occupational safety practices.
The table 3 shows that knowledge level of nurses regarding occupational hazards were, age between 21-25 yrs low level 72 (91.14) high level 59 (83.10) total 131, 26+yrs low level 7 (8.86) high level 12 (16.90) total 19 and chi-square 2.1854, p-value 0.1393. Between sex group in male low level 24 (30.38) high level 18 (25.35) total 42, female Low level 55 (69.62) high level 153 (74.65) total 108, chi-square 0.4688 and p-value 0.4935.
According to marital status unmarried low level 68 (86.08) high level 57 (80.28) total 125, married low level 11 (13.92) high level 14 (19.72) total 25, chi-square 0.9039 and p-value 0.3147. Level of education diploma low level 72 (91.14) high level 65 (91.55) total 137, bachelors low level 7 (8.86) high level 6 (8.45) total 13, chi-square 0.0079 and p-value 0.9290.
Designation of in charge low level 6 (7.59) high level 12 (16.90) total 18, senior staff nurse low level 7 (8.86) high level 7 (9.86) total 14, junior staff nurse low level 66 (83.54) high level 52 (73.24) total 118, chi-square 3.2436 and p-value 0.1976. Experience of 1-5yrs low level 76 (96.20) high level 64 (90.14) total 140, 6+yrs low level 3 (3.80) high level 7 (9.86) total 10, chi-square 2.2082 and p- value 0.1373.
Any training of yes low level 15 (18.99) high level 11 (15.49) total 26, no low level 64 (81.01) high level 60 (84.51) total 124, total low level 79 (100.00) high level 71 (100.00) total 150, chi-square 0.3187 and p-value was 0.5724.
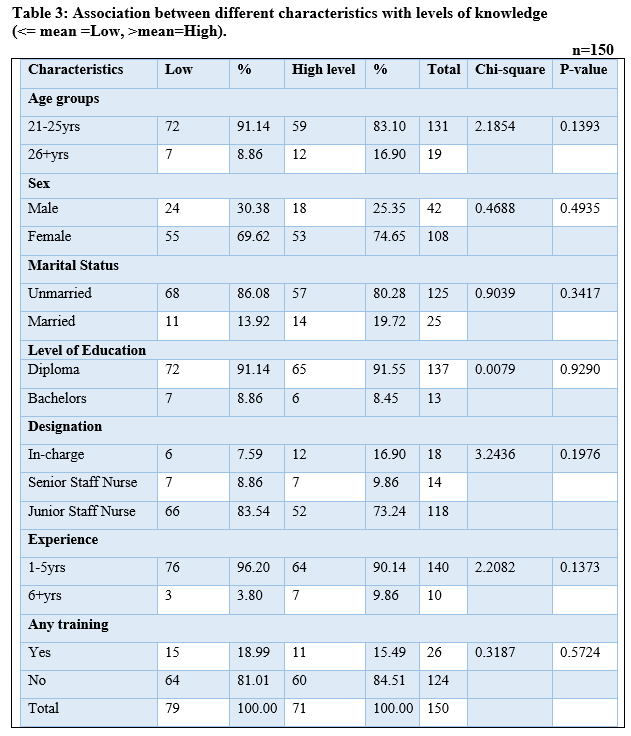
Note: Knowledge and practice levels were categorized using the mean score as the cutoff. Scores ≤ mean were classified as Low and scores > mean were classified as high.
The table 5 shows that practice level of nurses regarding occupational hazards were between age 21-25yrs low level 77 (97.47) high level 54 (76.06) total 131, 26+yrs low level 12 (15.19) high level 7 (9.86) total 19, chi-square 0.1319 and p-value 0. 7165. Sex group of male low level 27 (34.18) high level 15 (21.13) total 42, female low level 62 (78.48) high level 46 (64.79) total 108, chi-square 0.5929 and p- value 0.4413.
According to marital status of unmarried low level 77 (97.47) high level 48 (67.61) total 125, married low level 12 (15.19) high level 13 (18.31) total 25, chi-square 1.5970 and p-value 0.2063. Level of education of diploma low level 83 (105.06) high level 54 (76.06) total 137 bachelors low level 6 (7.59) high level 7 (9.86) total 13. Chi-square1.0246 and p-value 0.3114.
Designation of in charge low level 10 (12.66) high level 8 (11.27) total 18, senior staff nurse low level 10 (12.66) high level 4 (5.63) total 14, junior staff nurse low level 69 (87.64) high level 49 (69.01) total 118, chi-square 0.9914 and p-value 0.6092. Experience of 1-5yrs low level 85 (107.59) high level 55 (77.46) total 140, 6+yrs low level 4 (5.06) high level 6 (8.45) total 10, chi-square 1.6597 and p- value 0.1977.
Any training of yes low level 12 (15.19) high level 14 (19.72) total 26, no low level 77 (97.47) 47 (66.20) total 124, total low level 89 (112.66) high level 61 (85.92) total 150, chi-square 2.2641 and p-value was 0.1324.
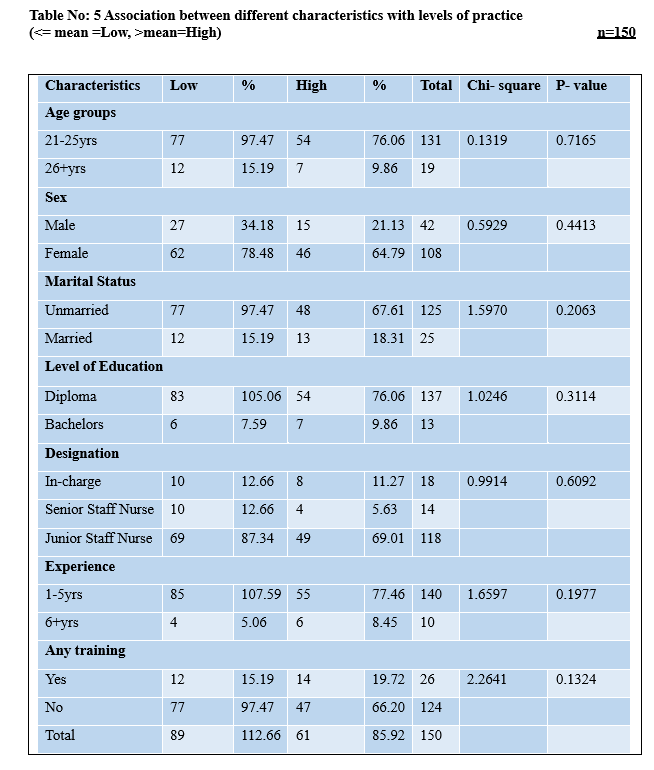
Note: Knowledge and practice levels were categorized using the mean score as the cutoff. Scores ≤ mean were classified as Low, and scores > mean were classified as High.
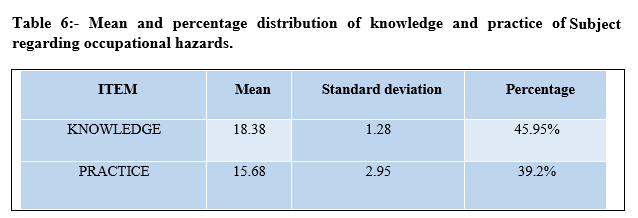
Table 6 shows that mean knowledge of the subjects were 18.38 (45.95%) with the standard deviation of 1.28 and the mean practice were 15.68 (39.2%) with the standard deviation of 2.95.
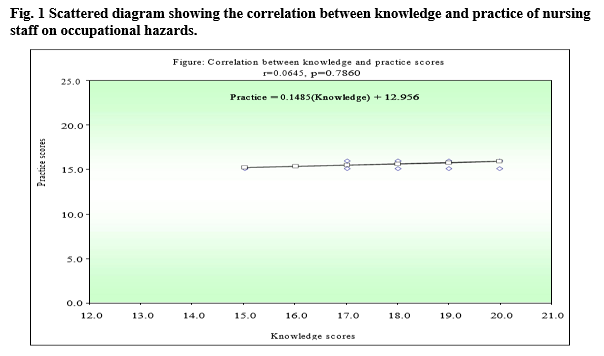
A scatterplot (Figure 1) demonstrated a weak positive correlation between knowledge and practice (r = 0.0645). This indicates that although knowledge is necessary, it does not consistently translate into safe practices.
DISCUSSION
This study highlights moderate knowledge and neutral practice levels among staff nurses regarding occupational hazards. The demographic profile—young, predominantly female, and early career—is consistent with findings from Iran (Razei et al.1) and India (Ashok, 2).
Despite relatively high knowledge scores, practice scores were lower, and the correlation between knowledge and practice was weak. This pattern mirrors findings from Nigeria (Amosu et al.5) and India (Senthil et al.7), where nurses demonstrated awareness but inconsistent application of safety measures.
The lack of significant associations between demographic variables and knowledge or practice suggests that occupational safety gaps are systemic rather than individual. The absence of training for most nurses (82.67%) is a critical concern, aligning with Alsabaani et al.9, who found that training significantly improves safety practices.
These findings underscore the need for structured, ongoing training programs, clear protocols, and consistent supervision to ensure that knowledge translates into safe practice.
CONCLUSION
Nurses demonstrated moderate knowledge and neutral practice levels regarding occupational hazards. Although a positive correlation exists between knowledge and practice, it is weak, indicating that knowledge alone is insufficient to ensure safe behavior.
To improve occupational safety:
• Structured orientation on occupational hazards should be mandatory at hiring.
• Regular in service training and refresher courses should be institutionalized.
• Continuous supervision and performance assessment are essential.
• A standardized learning package on occupational hazard prevention should be implemented.
Strengthening these components can enhance both knowledge and practice, ultimately improving workplace safety and patient care quality.
REFERENCES:
1. Razei S, Rad NR, Tamizi Z, et al. An investigation into occupational hazards faced by nurses in pediatrics hospitals of Tehran University of Medical Sciences. International Journal of Community Based Nursing and Midwifery. 2013;1:200–207.
2. Ashok D. Occupational hazards of medical group of women employees in healthcare units in Tamil Nadu, India. Journal of Business Management. 2012 Jul-Aug;2:44–45.
3. Mossburg S, Agore A, et al. Occupational hazards among healthcare workers in Africa: a systematic review. Annals of Global Health. 2019;85(1):78.1–13.
4. Juma LAK, Damian DJ, Njau B. Prevalence of occupational injuries and knowledge of availability and utilization of post-exposure prophylaxis among healthcare workers in Singida District Council, Singida Region, Tanzania. 2018.
5. Amosu AM, Degun AM, Atulomah NOS, Olanrewju MF, et al. The level of knowledge regarding occupational hazards among nurses in Abeokuta, Ogun State, Nigeria. Journal of Biological Sciences. 2011;86–90.
6. Al-Khatib IA, El Ansari W, et al. Occupational safety precautions among nurses at four hospitals in Nablus District, Palestine. International Journal of Occupational and Environmental Health. 2015;6:243–246.
7. Senthil A, Anandh B, Jayachandran P, et al. Perception and prevalence of work-related health hazards among healthcare workers in public health facilities in India. International Journal of Environmental Health. 2015;21.
8. Amare TG, Tesfaye TT, et al. Exposure to occupational health hazards among nursing and midwifery students during clinical practice. Risk Management and Healthcare Policy. 2021;14:2211–2220.
9. Alsabaani A, Alqahtani NSS, et al. Incidence, knowledge, attitude and practice toward needle stick injury among healthcare workers in Abha City, Saudi Arabia. Frontiers in Public Health. 2022;10.
10. Khamtuikrua C, Suksompong S. Awareness about radiation hazards and knowledge about radiation protection among healthcare personnel: a quaternary care academic center–based study. SAGE Open Medicine. 2020;8:1–8.