Feasibility of Brief Sleep Screening in Primary Care: A Rural Medical Track Quality Improvement Project
Joshua LaMar, OMS-IV, Oklahoma State University Center for Health Sciences, College of Osteopathic Medicine, Rural Medical Track
Krista Schumacher, PhD, Oklahoma State University Center for Health Sciences, Center for Rural Health
Corresponding Author:
Joshua LaMar, OMS-IV
(918) 344 8410
joshua.lamar@okstate.edu
Oklahoma State University College of Osteopathic Medicine
Disclosures: This work was partially funded by the Health Resources and Services Administration’s Medical Student Education Training Program (Grant T99HP52102). There are no conflicts of interest to disclose.
Background
Sleep difficulties affect a significant number of U.S. adults, making sleep a public health priority. However, clinical screening for sleep problems is uncommon, especially in the primary care setting.
Methods
This quality improvement project assessed the feasibility of screening adult primary care patients for sleep habits and perceived sleep difficulty during a 4-week medical student rotation. Under the direction of Family Medicine resident physicians, the student screened patients using an internally developed instrument. Screening time, documentation of results, and resident participation were tracked.
Results
Of 10 residents the medical student worked with, eight permitted screening, with half documenting results in the patient note. On average, screening took about 5 minutes. All 23 patients invited to participate consented, with 48% reporting occasional or daily problems sleeping, and 55% indicating trouble falling or staying asleep or both.
Conclusion
This study demonstrates that sleep screening may be feasible during primary care visits. Patient results point to the need for such screening, while resident engagement suggests most providers may be willing to screen for sleep issues. This project contributes to the growing emphasis on sleep as a public health priority.
Keywords: Sleep hygiene, sleep problems, quality improvement, sleep quality screening, public health, medical education
Introduction
It is estimated that over half of the American population struggled with sleep difficulties in 2015.1 Initial intervention for patients with sleep difficulties and disorders should involve behavioral and lifestyle modifications. A focus on sleep hygiene is one way to address sleep habits.2 Sleep hygiene can be defined as “a set of behavioral and environmental recommendations intended to promote healthy sleep.”1
Sleep disturbances are prevalent in the U.S. currently. A survey conducted by the American Academy of Sleep Medicine found that more than a quarter of adults did not achieve the recommended daily sleep duration.3 Additionally, the 2020 National Health Interview Survey revealed that 14.5% of adults across all age groups struggled with sleep on most nights of the week.3 Oklahoma ranks as one of the states with the highest percentage of residents with sleep difficulty, at 14.3% of the population.4
A particular concern for public health policy in Oklahoma should be increasing the knowledge about sleep, or sleep literacy, among the state's citizens. The relationship between low SES and low health literacy is well-documented.5 The average poverty rate in Oklahoma is higher than the overall national rate at 15.3%, compared with 12.4%.6 It is also significant to note that the majority of Oklahoma’s 77 counties have worse outcomes than the national average as it pertains to the rate of people who live in poverty.6 Sleep, like overall health, is influenced by social determinants of health.7
Primary care physicians are well-positioned to assess patients for sleep disturbances. This could be done during the initial visit and repeated at regular intervals going forward. The lack of screening was demonstrated in a study by Senthilvel et al., which showed that while sleep problems are common, they are not routinely screened for by primary care physicians.8 One reason for this is the lack of screening recommendations by the USPSTF regarding sleep.8,9 One reason is thought to be the perceived time it takes away from a patient visit.8 However, it has been previously hypothesized that screening for sleep-related disorders can be accomplished with a single question.10 There is a benefit in discussing sleep with a patient. Although an immediate solution to a patient’s insomnia may not be found, having the conversation can help improve patient rapport and deepen the physician-patient relationship.7,11
Sleep is essential for completing regular daily activities and properly regulating mood.2 Due to the prevalence of sleep difficulty in Oklahoma and across the country, specific attention should be given to the use of maladaptive compensatory behaviors and adverse events due to sleep deprivation.12 On the individual level, impaired sleep affects the physiology of the human body by increasing the risk of metabolic, cardiovascular, and psychological diseases, as well as impairing memory formation and immune system function.2
Common lifestyle factors that impact sleep include caffeine consumption, nicotine use, alcohol consumption, decreased physical activity, inadequate stress management, and irregular sleep patterns.1 When sleep problems persist, individuals may turn to substances such as alcohol, antihistamines, benzodiazepines, and barbiturates, although these can negatively impact sleep quality or other physiological processes.2 While data on the clinical efficacy of sleep hygiene as a single treatment method is lacking, the importance of sleep hygiene education should not be understated.1
There are many approaches to sleep dysfunction in society currently. Sleep disorder management is based on the etiology of the disorder. The initial approach to diagnosing sleep dysfunction involves clinical screening using indices such as the Epworth Sleepiness Scale and the Pittsburgh Sleep Quality Index.13,14 These tools are primarily used to evaluate symptoms suggestive of sleep disorders, after which diagnostic tools such as polysomnograms may be used to diagnose a sleep disorder.
The prevalence of sleep disturbances nationwide underscores the need for screening and educating patients on maintaining good sleep habits. By addressing the growing number of people struggling with sleep, primary care physicians may be able to address other health conditions that are common sequelae of sleep deprivation.
The purpose of this project is to assess the feasibility of screening patients’ sleep hygiene practices during a regular clinic visit. This project aims to gain insight into expanding the conversation about sleep and the follow-up steps that could be taken to address sleep hygiene in patients, particularly those from low-SES backgrounds.
Methodology
This project was implemented as part of a four-week community clinic rotation at the Family First Clinic, part of the Lawton Community Health Center (LCHC), a Federally Qualified Health Center in Lawton, Oklahoma. The Family First Clinic serves as the continuity clinic for the Memorial Health System of Southwest Oklahoma Family Medicine Residency Program. Per OSU-CHS Institutional Review Board guidance, QI projects solely intended to improve health outcomes do not qualify as human subjects research;15 therefore, this project was not submitted for IRB approval. The medical student obtained approval from the Residency Program Director before initiating screenings.
After reviewing common factors that affect sleep,1,2 the medical student and a resident physician developed a brief structured set of questions to guide discussion of sleep habits during patient visits. The goal was to provide a set of questions that could easily be incorporated into a primary care visit without taking time away from the reason for the visit. No items were adapted from existing screeners. The resident physician reviewed items to ensure they reflected typical clinical questions used when discussing sleep habits with patients. The question set consisted of ten prompts designed to explore patients’ sleep patterns and sleep hygiene. Items addressed sleep difficulty, sleep duration, bedtime routine, afternoon and evening activities, and efforts to improve sleep quality, such as using sleep aids.
Patients were under the care of resident physicians, and patient selection was determined by the residents, daily clinic flow, and patient interest in participating. Exclusion criteria included patients younger than 18 or presenting for a complex visit, such as those lasting longer than 30 minutes. Screening was conducted only during uncomplicated visits. If screening could potentially delay the resident, then it was not conducted; thus, at no time were residents delayed in providing care. At the end of the student’s part of the visit, before the resident entered the room, patients were invited to describe their sleep habits, and the screening questions served as prompts to guide the conversation without categorizing responses as healthy or problematic during the screening. The student did not coach patients or interpret responses during the discussion. Any clinical interpretation or follow-up recommendations were left to the resident physician.
The student documented screening duration and responses, and the resident decided whether to incorporate this data into the patient note. Residents amenable to screening were informed of results during the student’s presentation of the patient, and responses were documented in the history of present illness section of the visit note at each resident’s discretion. Some residents chose to include patient responses in the HPI, while others simply noted an assessment had been given or chose to eliminate any mention of screening from the patient note. After the visit, the student transcribed responses into a password-protected Google Sheet accessible only to the medical student. All data were de-identified.
Results
All patients invited to participate consented, and screening was well-received by patients and most residents. In total, 23 patients were screened during the rotation. Screening occurred on at least eight of the 13 clinic days the student was present during the rotation. At most, four patients were screened in a single day. The tables below present the results of the study.
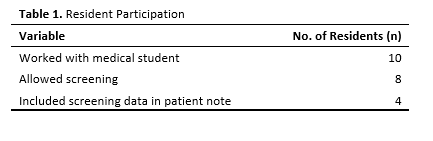
Participants were about evenly split between those younger than 50 years and 50 or older, with slightly more female than male patients (14 versus 9, respectively). Of 10 residents the medical student worked with during the rotation, eight (80%) were willing to have their patients included in the study. Of these, four (50%) included information from the screening in the patient note (see Table 1).
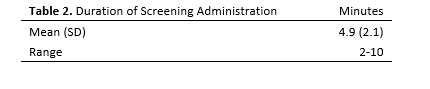
On average, asking patients about their sleep took about 5 minutes, with a standard deviation of 2.1 minutes and a range of 2-10 minutes (see Table 2). The recorded screening duration excludes time spent informing residents of the results. The questions provided a good guide for discussing patients’ sleep habits and were manageable within the student’s portion of the clinical visit.
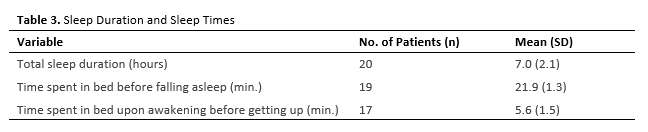
Patients slept an average of 7 hours at a time, with about 21 minutes spent falling asleep and nearly 6 minutes spent waking up before rising (see Table 3).
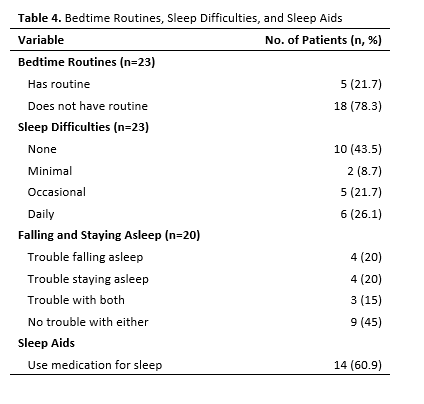
Patients reported varying bedtime routines and sleep difficulties, as shown in Table 4. Most patients (78%) reported having no routine before bed. Nearly half (48%) of patients reported occasional or daily problems sleeping, and 55% reported trouble falling or staying asleep or both. In addition, 61% reported using medications to aid sleep. An anecdotal finding was that two patients reported significantly improved sleep quality after adopting lifestyle changes that promote healthy sleep hygiene.
Discussion
This project sought to assess the feasibility of screening patients for sleep hygiene practices in the primary care setting. All patients invited to participate consented to screening, suggesting an openness to discussing sleep issues.
While not intended to diagnose sleep disorders, the questions offered an efficient way to demonstrate provider concern and raise awareness of sleep health, a topic often overlooked in routine care.8 Its short duration left time to address patients’ sleep-related concerns without detracting from the purpose of the visit. The screener’s ease of use may make it ideal for busy clinical settings where longer and more complex instruments are impractical.
This project had several limitations. Not all patients were given the opportunity to participate, as screening depended on resident willingness and visit complexity. Clinic delays and a large pediatric population also limited the sample size. The screener itself was developed in-house and not tested against validated tools, so its reliability and validity as a measure of poor sleep habits is unknown. Because no follow-up data were collected, it is also unknown if screening led to sustained behavior change or improved sleep.
Resident physician engagement varied. Most residents permitted screening, with some ensuring all of their patients were screened, while others opted out due to limited interest or concerns about time. Half of participating residents recorded screening results in patient notes, while the other half preferred to keep notes relevant to the visit purpose. While inconsistent documentation limited assessment of how results were used, the inclusion of some results in patient records suggests screening data can easily be included and potentially discussed in future visits.
Overall, the project received significant support from residents, clinic staff, and the residency program director, who expressed interest in advancing the initiative. Taken together, the findings suggest that brief screening may provide a practical way to initiate conversations about sleep health in the primary care setting.
Conclusion
Many patients were dissatisfied with their current sleep quality and expressed little understanding of good sleep hygiene, underscoring the need for routine screening and education in the primary care setting. This QI project suggests that brief screening tools may help initiate conversations about sleep health during primary care visits.
Since this project excluded pediatric patients, future research could explore whether screening and education help identify problems and improve sleep across a broader range of ages.
Future studies could evaluate whether sleep screening and education improve patient awareness of good sleep habits. Additional research may also explore how brief screening tools can be incorporated into clinical workflows across diverse primary care settings.
Acknowledgements
A special thank you to Mercedez Bernard, DO, residency program director, and Ariana Harwood, DO, family medicine resident physician, for their support in completing this project.
References
1. Irish LA, Kline CE, Gunn HE, Buysse DJ, Hall MH. The role of sleep hygiene in promoting public health: a review of empirical evidence. Sleep Med Rev. 2015;22:23-36. doi:10.1016/j.smrv.2014.10.001
2. Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis. 2023;77:59-69. doi:10.1016/j.pcad.2023.02.005
3. Adjaye-Gbewonyo D, Ng AE, Black LI. Sleep Difficulties in Adults: United States, 2020. National Center for Health Statistics; 2022. doi:10.15620/cdc:117490
4. Grandner MA, Smith TE, Jackson N, Jackson T, Burgard S, Branas C. Geographic distribution of insufficient sleep across the United States: a county-level hotspot analysis. Sleep Health. 2015;1(3):158-165. doi:10.1016/j.sleh.2015.06.003
5. Coughlin SS, Vernon M, Hatzigeorgiou C, George V. Health literacy, social determinants of health, and disease prevention and control. J Environ Health Sci. 2020;6(1):3061. https://pmc.ncbi.nlm.nih.gov/articles/PMC7889072/
6. Poverty Table for Oklahoma Counties. HDPulse Data Portal. Accessed February 5, 2026. https://hdpulse.nimhd.nih.gov/data-portal/social/table?age=001&age_options=ageall_1&demo=00008&demo_options=poverty_3&race=00&race_options=race_7&sex=0&sex_options=sex_3&socialtopic=080&socialtopic_options=social_6&statefips=40&statefips_options=area_states
7. Dunietz GL, Jansen EC, Chervin RD. What should a public health approach to sleep look like? AMA J Ethics. 2024;26(10):795-803. doi:10.1001/amajethics.2024.795
8. Senthilvel E, Auckley D, Dasarathy J. Evaluation of sleep disorders in the primary care setting: History taking compared to questionnaires. J Clin Sleep Med. 2011;7(1):41-48. https://pmc.ncbi.nlm.nih.gov/articles/PMC3041630/
9. Prevention Task Force Search. U.S. Preventive Services Task Force. Accessed December 3, 2025. https://www.uspreventiveservicestaskforce.org/webview/#!/
10. Kuppermann M, Lubeck DP, Mazonson PD, et al. Sleep problems and their correlates in a working population. J Gen Intern Med. 1995;10(1):25-32. doi:10.1007/BF02599573
11. Moloney ME, Konrad TR, Zimmer CR. The medicalization of sleeplessness: A public health concern. Am J Public Health. 2011;101(8):1429-1433. doi:10.2105/AJPH.2010.300014
12. Worley SL. The extraordinary importance of sleep. P T. 2018;43(12):758-763. https://pmc.ncbi.nlm.nih.gov/articles/PMC6281147/
13. Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep. 1991;14(6):540-545. doi:10.1093/sleep/14.6.540
14. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Research. 1989;28(2):193-213. doi:10.1016/0165-1781(89)90047-4
15. Oklahoma State University Center for Health Sciences. HRP-820 investigator guidance: Quality improvement activities in health care. Human Subjects Research, Investigator Guidance. January 28, 2019. Accessed October 31, 2025. https://medicine.okstate.edu/research/human-subjects-research/hrp/hrp-820-investigatorguidance-quality-improvement-activities.pdf