Accidental Camphor Ingestion in a Patient with Seizure Disorder: A case report
Gabrielle D. Smith, BS., Oklahoma State University Center for Health Sciences,
1111 W. 17th St, Tulsa, OK 74107
Alexandra G. White, BS., Oklahoma State University Center for Health Sciences,
1111 W. 17th St, Tulsa, OK 74107
Aaron Lane, DO., Department of Emergency Medicine, Oklahoma State University Center for Health Sciences, 1111 W 17th St, Tulsa, OK 74107
Kelly A. Murray, PharmD ., Department of Emergency Medicine, Oklahoma State University Center for Health Sciences, 1111 W 17th St, Tulsa, OK 74107
Disclosure statement: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Funding Statement: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Camphor is a highly lipophilic bicyclic monoterpene ketone used topically for temporary pain relief, itching, cough, and nasal congestion 1. Acting through transient receptor potential channels 1/2 (TRPV1/TRPA2), camphor produces local pain relief by desensitizing sensory neurons 2. Additionally, it’s available over the counter as a liquid and can be combined with other ingredients such as phenol for antiseptic purposes 3. Directions instruct the user to add one tablespoon of solution per quart of water when used in a steam vaporizer. Manufacturers emphasize the need for immediate medical assistance if swallowed as it is meant for inhalation only. 4
Despite its wide availability, camphor is a known neurotoxin. In 1983, the FDA regulated that products with camphor concentration cannot exceed 11% as it can rapidly lead to seizures, lethargy, ataxia, severe nausea, vomiting, CNS depression, and mental status changes.5 The American Association of Poison Control Centers suggests an emergency department referral for any patient with severe symptoms or an ingestion over 30 mg/kg of camphor-containing products, such as medicated vaporizing steam liquid. Treatment of camphor-induced seizures in the emergency department should include prompt administration of benzodiazepines as first-line therapy. 5
We present a case of accidental camphor overdose with associated camphor product concentrations, the care required for evaluation and medical management of camphor overdose, and concerns for similarities in packaging and labeling between over-the-counter product options.
Case Report:
A 53-year-old female (112.49 kg) presented to an urban emergency department (ED) by ambulance after accidental ingestion of an estimated 4 ounces of 6.2% camphor oil humidifier solution (6.2 grams of camphor per 100 mL). After experiencing constipation for many days, she reports confusing the bottle for magnesium citrate and did not immediately notice the difference due to holding her nose in attempt to mask the taste. En route to the hospital, the patient experienced nausea and vomiting. The patient brought in the product consumed and the care team calculated the estimated total number of grams ingested for this patient to be between 8.7 to 10.4 grams (77.5 to 92.4 mg/kg) based on the solution remaining in the bottle. Her medical history was significant for a seizure disorder secondary to brain tumor with recent brain tumor removal, diffuse large B-cell lymphoma, previous pulmonary emboli, hypertension, and COPD. Relevant home medications for the patient include lacosamide, levetiracetam, gabapentin, and bupropion. Initial vital signs were pulse 122 bpm, blood pressure 137/78 mmHg, temperature 37°C, and oxygen saturation 94% on room air.
After initial examination, anxious, jittery symptoms were reported by the patient, prompting 2 mg of lorazepam to be given intravenously in an attempt to raise her seizure threshold. She was also given 1L of intravenous 0.9% sodium chloride solution. An initial complete blood count (CBC) revealed a white blood count (WBC) of 7, low hemoglobin of 10 with a hematocrit of 33.4, and a normal platelet count of 184,000. A complete metabolic panel (CMP), total creatine kinase (CK), ammonia, troponin, and thyroid stimulating hormone (TSH) levels were all within normal limits. The urinalysis was normal, and her serum and urine drug screen were positive for marijuana and amphetamine, possibly from her home medication bupropion, known for causing false positives.
The electrocardiogram showed sinus tachycardia with no other abnormalities.
Due to the patient’s history of seizures and consultation with the poison control center, the patient was admitted for observation and monitored for seizure activity. While inpatient, she remained asymptomatic with unchanged labs. She was discharged after an overnight stay and had no severe adverse effects from the unintentional ingestion of camphor.
Discussion:
Camphor overdose typically presents with rapid onset of gastrointestinal (nausea, vomiting), neurologic (headache, irritability, convulsions, lethargy, ataxia), and pulmonary (respiratory depression, apnea) symptoms. Though ingestions of 30 mg/kg raise concern, research suggests doses over 50 mg/kg can be neurotoxic and 500 mg/kg fatal. 6 This patient was at risk of neurotoxicity based on her weight-based ingestion dose. Most cases of camphor poisoning resolve by 24-48 hours but, on occasion, toxic effects may persist due to axonal hyperexcitability or continued camphor release from fat stores. 7
Convulsions could occur as early as 30 minutes following ingestion, but those who are asymptomatic at 4 hours are unlikely to develop toxicity 5. Patients may also demonstrate moderate elevations in hepatic transaminases (AST, ALT) and evidence of renal toxicity; therefore, monitoring is warranted 8.
No published literature currently addresses camphor toxicity in individuals with a preexisting seizure disorder. Camphor ingestion has been reported in the pediatric population, particularly among families who use it in cultural practices. However, these exposures are likely under-reported by caregivers 9. This mechanism of toxicity should be considered with patients who present with new onset seizures of unknown origin. This patient’s treatment plan included monitoring and proactively preventing seizure activity by administering lorazepam after initial examination as well as home seizure medications, with follow up observation.
The circumstances leading to this exposure highlight a critical public health issue regarding the labelling of over-the-counter (OTC) products 10. This patient’s intention was to ingest magnesium citrate for constipation but mistakenly consumed a large quantity of camphor solution intended for use in a humidifier, citing the generic branded bottles looked similar (Figure 1). Manufacturers should prioritize distinct packaging and labeling strategies to reduce visual similarity among consumer health products, particularly those with clear liquid formulations and serious consequences when ingested. Furthermore, healthcare providers should counsel patients to store OTC medications and liquids not for human consumption separately.
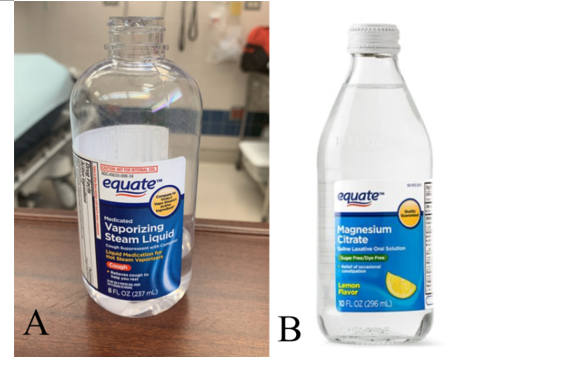
Figure 1. (A) Patient’s medicated vaporizing steam liquid cough suppressant with camphor. (B) over-the-counter Magnesium citrate saline laxative.
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Ultimately, this case illustrates a unique scenario of unintentional camphor overdose in a patient with a known seizure disorder and calls for emergency department physicians and healthcare providers to consider camphor overdose in patients who present with seizures after a presumed magnesium citrate ingestion. It also reinforces the need for improved product differentiation and public education to prevent similar toxic ingestion, as well as appropriate ED management of camphor toxicity utilizing proper medications for seizure prophylaxis. Preventing such events requires both clinical preparedness and public education, both paramount in effective poisoning prevention.
References:
1. Chen W, Vermaak I, Viljoen A. Camphor--a fumigant during the Black Death and a coveted fragrant wood in ancient Egypt and Babylon--a review. Molecules. 2013;18(5):5434-5454. Published 2013 May 10. doi:10.3390/molecules18055434
2. Xu H, Blair NT, Clapham DE. Camphor activates and strongly desensitizes the transient receptor potential vanilloid subtype 1 channel in a vanilloid-independent mechanism. J Neurosci. 2005;25(39):8924-8937. doi:10.1523/JNEUROSCI.2574-05.2005
3. Mathen PG, Sreekrishnan TP, Kumar KPG, Mohan N. Camphor poisoning: A rare cause of acute symptomatic seizures in children. J Emerg Trauma Shock 2018;11(3):228-229.
4. Campho-Phenique Antiseptic (camphor-synthetic and phenol gel). DailyMed. U.S. National Library of Medicine. Updated December 2, 2024. Accessed August 26, 2025.
5. Manoguerra AS , Erdman AR, Wax PM, et al. Camphor Poisoning: an evidence-based practice guideline for out-of-hospital management. Clin Toxicol (Phila). 2006;44(4):357-70.
6. Kumar S, Kavitha TK, Angurana SK. Kerosene, camphor, and naphthalene poisoning in children. Indian J Crit Care Med. 2019;23(Suppl 4):S278–S281. doi:10.5005/jp-journals-10071-23316
7. Santos CD, Cabot JC. Persistent effects after camphor ingestion: a case report and literature review. J Emerg Med. 2015;48(3):298-304. doi:10.1016/j.jemermed.2014.05.015
8. Antman E, Jacob G, Volpe B, et al. Camphor overdosage. Therapeutic considerations. N Y State J Med 1978; 78:896.
9. Khine H , Weiss D, Graber N, Hoffman RS, Esteban-Cruciani N, Avner JR. A cluster of children with seizures caused by camphor poisoning. Pediatrics 2009;123(5):1269-72.
10. Bryan R, Aronson JK, Williams A, Jordan S. The problem of look-alike, sound-alike name errors: Drivers and solutions. Br J Clin Pharmacol. 2021 Feb;87(2):386-394. doi: 10.1111/bcp.14285. Epub 2020 Apr 20. PMID: 32198938.