Patient Education on Nonopioid Pain Management in Primary Care: A Quality Improvement Project
Gilbert Che, OMS-III, Oklahoma State University Center for Health Sciences, College of Osteopathic Medicine at Tulsa
Krista Schumacher, PhD, Oklahoma State University Center for Health Sciences, Center for Rural Health
Corresponding Author:
Gilbert Che, OMS-III
(580) 890-0164
giche@okstate.edu
OSU College of Osteopathic Medicine at Tulsa
Disclosures: This work was partially funded by the Health Resources and Services Administration’s Medical Student Education Training Program (Grant T99HP52102). There are no conflicts of interest to disclose.
Abstract
Background
Chronic pain is frequently managed with opioid therapy despite known risks and limitations, and rural populations have experienced disproportionate opioid-related morbidity and mortality. Given this burden, increasing awareness of nonopioid pain management strategies is needed. Patient education may support patient-centered decision making and consideration of opioid alternatives. This quality improvement project, conducted during a four-week clinical rotation, evaluated whether brief education increased awareness of nonopioid options, perceived control over pain management, and interest in nonopioid approaches.
Methods
Adult patients receiving opioid therapy for chronic pain at a rural primary care clinic received brief education on nonopioid pharmacologic and nonpharmacologic options during routine visits. Anonymous post-intervention surveys assessed awareness of alternatives, perceived control over pain, and interest in opioid reduction. Descriptive statistics were calculated.
Results
Eight patients completed surveys. All reported increased awareness of alternatives. Most reported increased perceived control (75%). Nearly 40% reported greater interest in nonopioid strategies, and 25% expressed interest in reducing opioid use.
Conclusions
Brief clinic-integrated education may increase perceived control over pain management and awareness of nonopioid alternatives. Such efforts may promote shared decision-making and multimodal pain management in rural primary care.
Keywords: opioid stewardship; rural health; primary care; multimodal pain management; quality improvement; patient education
Introduction
Chronic pain affects a considerable portion of the U.S. population, with approximately 21% of adults living with chronic pain and nearly 7% suffering from high-impact chronic pain that limits daily activities.1 As a leading cause of disability and one of the most common reasons for seeking medical care, chronic pain has contributed to substantial opioid prescribing despite limited evidence supporting the long-term benefits of opioid therapy.2–4 Recent years have seen declines in opioid prescribing across the nation, yet long-term opioid therapy continues to be common, leading to greater risks for opioid use dependence, misuse, and overdose.2,3 In addition, prescription opioid use has been associated with subsequent use of illicit synthetic opioids, now largely responsible for opioid-related mortality in Oklahoma and nationally.5–7
Relative to urban areas, rural communities have experienced disproportionate harm from opioids, including higher rates of nonmedical prescription opioid use and associated adverse outcomes.8 In 2024, Oklahoma had approximately 50.9 opioid prescriptions dispensed per 100 persons, one of the highest rates in the nation and exceeding the national average of 35.4 per 100 persons.9 Largely rural states like Oklahoma are particularly vulnerable to opioid-related morbidity and mortality due in part to higher rates of opioid prescribing in rural areas and economic stressors that increase susceptibility to drug use.8,10,11 Improving chronic pain management remains a public health priority, particularly in rural communities.2,8
Clinical practice guidelines recommend prioritizing nonopioid and multimodal, patient-centered approaches for chronic pain management. For example, the 2022 CDC Clinical Practice Guideline for Prescribing Opioids for Pain emphasizes the use of nonpharmacologic and nonopioid therapies and stresses the need for providers to carefully weigh the risks and benefits of opioid therapy before starting or continuing such treatments.2 The American College of Physicians recommends approaches such as exercise therapy, cognitive behavioral therapy, and multidisciplinary rehabilitation as first-line treatments for chronic low back pain.12
Despite evidence pointing to the effectiveness of opioid alternatives in decreasing pain and improving daily functioning,3,11long-term opioid therapy remains common.8 Barriers to implementing nonopioid strategies in primary care include limited access to multidisciplinary services, such as pain management specialists; insurance constraints, especially for nonpharmacologic therapies; time pressures within routine clinical encounters; and reluctance of patients to transition off opioids.2,11,13 In rural areas where access to nonpharmacologic services is limited, these challenges may be particularly pronounced.10
Efforts to advance safer pain care, such as reducing reliance on opioid therapy, include patient education and shared decision-making. Supporting self-management through patient education has been found to improve pain-related outcomes,14 while shared decision-making enhances patients’ understanding of available options and encourages participation in treatment decisions.15 However, evidence on the feasibility or efficacy of such approaches, especially in rural clinical settings, is limited. The role of routine primary care interactions in increasing awareness of opioid alternatives and enhancing patients’ perceived control over pain management remains understudied.16
The purpose of this quality improvement project was to evaluate whether brief patient education with adults receiving opioid therapy in a rural primary care clinic increased awareness of nonopioid pain management strategies, perceived control over pain management, and interest in nonopioid options.
Methods
This project was conducted as part of a four-week family medicine clinical rotation at Park Clinic Family Care in Duncan, Oklahoma during the fall of 2025. The clinic is a designated Rural Health Clinic (RHC) and part of the Duncan Regional Hospital Health System. The project was reviewed and determined not to meet the criteria for human subjects research by the OSU-CHS Institutional Review Board (IRB #2025103).
Adult patients with chronic pain who reported regular opioid use were asked during routine visits whether they would be interested in learning about alternatives to opioids. At the end of the visit, the clinician informed patients who agreed to participate that additional information about nonopioid pain management would be provided and then exited to complete visit documentation.
The medical student provided brief education lasting approximately three to five minutes. The discussion was guided by a printed handout listing nonopioid pharmacologic options, such as acetaminophen and nonsteroidal anti-inflammatory medications, and nonpharmacologic pain management strategies, such as exercise, physical therapy, and other lifestyle modifications. The student responded to patient questions and gave them the handout for future reference. Patients were encouraged to talk to their primary care provider if they had further questions or were interested in pursuing any of the alternatives discussed. No changes were made to patients’ current opioid prescriptions.
Immediately after the discussion, patients completed a short paper survey assessing pain manageability, awareness of alternative pain management strategies, perceived control over pain, interest in nonopioid approaches, and intentions related to opioid reduction. No identifying data were collected. Survey responses were analyzed using descriptive statistics.
Results
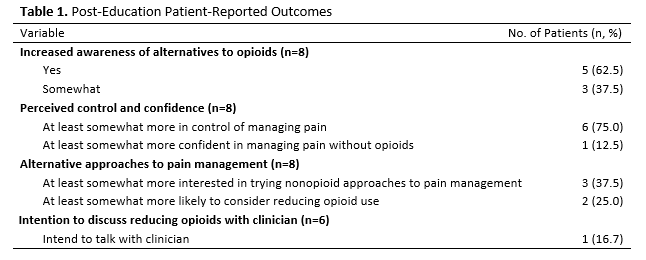
Eight patients agreed to participate and completed the post-intervention survey (see Table 1). All respondents reported at least some increase in awareness of nonopioid pain management strategies following education. Most participants (75%) reported feeling at least somewhat more in control of managing their pain after learning about alternative approaches. Only one participant (12.5%) reported increased confidence managing pain without opioids.
Interest in nonopioid strategies was modest. Nearly 40% reported being at least somewhat more interested in trying nonopioid strategies, and 25% expressed increased interest in reducing opioid use. Among the six respondents who answered the question regarding discussing opioid reduction with their clinician, one (16.7%) reported being more likely to do so.
Discussion
Although interest in reducing opioid use was limited, this project found that brief patient education was associated with increased awareness of opioid alternatives and greater perceived control over managing pain. This finding aligns with the literature on shared decision-making, which posits that before changing treatment plans, patients must first understand their choices.15 According to self-management theory, concrete behavioral changes are often preceded by improvements in perceived control and self-efficacy.14 Although confidence in managing pain without opioids changed minimally, increases in awareness and perceived control may represent earlier stages of behavioral change.
The findings also suggest that integrating brief conversations into routine primary care visits without altering prescribing practices or disrupting clinic workflow may be feasible. All patients approached agreed to participate, pointing to an openness to discussing nonopioid strategies. Education required minimal time during clinic visits and did not detract from other clinical responsibilities.
This project had a few limitations, including a small sample size, use of a single clinical site, short duration, and reliance on self-reported outcomes, which may have introduced social desirability bias. Despite these limitations, integrating short conversations into routine visits may be a practical way to expand awareness of nonopioid options. Future studies could evaluate whether ongoing education, such as repeated or sustained efforts over time, contributes to measurable changes in opioid prescribing patterns and patient behavior.
Conclusion
Opioid-related morbidity and mortality remain public health concerns. This project suggests that even brief, structured patient education during routine primary care visits may support patient-centered multimodal pain management and opioid stewardship in rural settings.
Acknowledgments
Thank you to the clinical staff at Park Clinic Family Care for their support of this project.
References
1. Zelaya CE, Dahlhamer JM, Lucas JW, Connor EM. Chronic pain and high-impact chronic pain among U.S. adults, 2019. NCHS Data Brief. 2020;(390):1-8.
2. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71(No. RR-3). doi:10.15585/mmwr.rr7103a1
3. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015;162(4):276-286. doi:10.7326/M14-2559
4. Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320(23):2448-2460. doi:10.1001/jama.2018.18472
5. Drug overdose data. Oklahoma State Department of Health. 2026. Accessed February 25, 2026. https://oklahoma.gov/health/health-education/injury-prevention-service/drug-overdose/data.html
6. Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2023–2024. NCHS Data Brief. 2026;549. doi:10.15620/cdc/174639
7. Dickson-Gomez J, Krechel S, Spector A, et al. The effects of opioid policy changes on transitions from prescription opioids to heroin, fentanyl and injection drug use: a qualitative analysis. Subst Abuse Treat Prev Policy. 2022;17(1):55. doi:10.1186/s13011-022-00480-4
8. Keyes KM, Cerdá M, Brady JE, Havens JR, Galea S. Understanding the rural-urban differences in nonmedical prescription opioid use and abuse in the United States. Am J Public Health. 2014;104(2):e52-59. doi:10.2105/AJPH.2013.301709
9. Centers for Disease Control and Prevention. United States Dispensing Rate Maps. Overdose Prevention. February 11, 2026. Accessed February 23, 2026. https://www.cdc.gov/overdose-prevention/data-research/facts-stats/us-dispensing-rate-maps.html
10. Baker MB, Liu EC, Bully MA, et al. Overcoming barriers: a comprehensive review of chronic pain management and accessibility challenges in rural America. Healthcare. 2024;12(17). doi:10.3390/healthcare12171765
11. Tick H, Nielsen A, Pelletier KR, et al. Evidence-based nonpharmacologic strategies for comprehensive pain care: The Consortium Pain Task Force White Paper. Explore (NY). 2018;14(3):177-211. doi:10.1016/j.explore.2018.02.001
12. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514-530. doi:10.7326/M16-2367
13. Crouch TB, Donovan E, Smith WR, Barth K, Becker WC, Svikis D. Patient motivation to reduce or discontinue opioids for chronic pain: self-efficacy, barriers, and readiness to change. Clin J Pain. 2024;40(1):18-25. doi:10.1097/AJP.0000000000001167
14. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1-7. doi:10.1207/S15324796ABM2601_01
15. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361-1367. doi:10.1007/s11606-012-2077-6
16. Becker WC, Bair MJ, Picchioni M, Starrels JL, Frank JW. Pain management for primary care providers: a narrative review of high-impact studies, 2014–2016. Pain Med. 2018;19(1):40-49. doi:10.1093/pm/pnx146