Comparison of Patient Knowledge and Perspectives on Herbal Therapies Before and After Pharmacist-Led Education
Abigail R. Birky, Pharm.D.; PGY-1 Community-Based Resident, Southwestern Oklahoma State University College of Pharmacy and Walgreen Co., Oklahoma City, OK, United States.
Nancy T. Williams, Pharm.D., BCPS, BCNSP, FASHP; Residency Program Director, Pharmacy Practice Department Chair, Southwestern Oklahoma State University College of Pharmacy, Oklahoma City, OK, United States.
Lisa Appeddu, Ph.D., Professor of Physiology, Southwestern Oklahoma State University College of Pharmacy, Weatherford, OK, United States.
Corresponding Author: Abigail Birky, Pharm.D.
Email: abigail.birky@walgreens.com
Disclosure of Funding: Walgreens provided Walgreens Cash Rewards and small promotional products as an incentive for participation. Abigail Birky is an employee of Walgreen Co.
Comparison of Patient Knowledge and Perspectives on Herbal Therapies Before and After Pharmacist-Led Education
Objectives: The aims of this study were (1) to characterize community pharmacy patients' baseline knowledge about, perspectives on, and use of herbal medications; (2) to examine to what degree patient demographics correlate with baseline responses; and (3) to assess if pharmacist-led education about herbal medicines changed patient behaviors and perspectives.
Methods: In this pre/post-survey study design, a 28-question pre-education survey was used to assess perceptions, use, and knowledge of select herbal medications. A convenience sample from five large-chain retail pharmacies in the Oklahoma City metro area of 21 English-speaking/reading patients 18 years of age or older were recruited to participate in the study. Following completion of the initial survey, an educational session in the form of a popular trivia game show was provided. Education provided information on 15 commonly used herbal medications, along with herbal supplement regulation and labeling requirements. After game completion, a 9-question post-survey was provided to the participants to assess the impact education had on their perspectives or future use of herbal medications.
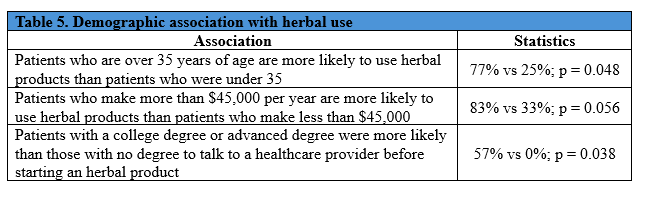
Results: The study found that 57% of participants had used herbal products, but less than half reported those to a prescriber. Patients who were over the age of 35 or made more than $45,000 a year were more likely to use herbal products (p = 0.048 and 0.056, respectively), and those with a college degree or higher level of education were more likely to report herbal use to a provider (p = 0.038). Participants were more likely to agree that reporting herbal use is important after pharmacist-led education (p = 0.025).
Conclusions: This study suggests that more than half of patients have used herbal medications, and that demographic factors may influence both the use of and patients’ knowledge of these products. Patients’ perceived importance of reporting herbal medications to a provider was increased after education was provided, indicating that pharmacists have a key role to play in this aspect of patient health.
Introduction
Herbal therapies are easily accessible and widely used by patients in the United States (U.S.). Unfortunately, not every patient understands the medications they are taking or that they should report the use of herbal products to their prescriber. Herbal products have been increasingly advertised on social media sites, but not every post or video about a product contains all the information a patient should know. For example, ashwagandha should not be used by pregnant women,1 and St. John’s wort has many drug interactions.2 Many patients may also be unaware that the Food and Drug Administration (FDA) does not regulate herbal products in the same way as over-the-counter medications because they are categorized as dietary supplements.3 Herbal products are not required to have proven efficacy, safety, or purity prior to going on the market and are only investigated by the FDA if there is an issue reported.
Using data from the 2012 National Health Statistics Report, Clarke et al.4 found that over 17% of adults in the U.S. were using some form of non-vitamin, non-mineral dietary supplements. In analyzing the same data, Nahin et al.5 found that there were more than 32 million individual expenditures for herbal medications by adults in a single year, generating 12 billion dollars in medical expenses annually. Additionally, in 2015, Gardiner et al.6 found that out of 33% of patients who admitted to using dietary supplements, only 18% said they had reported them to a physician or healthcare provider. Despite this high use and impact on the healthcare field, patient knowledge and perspectives on using herbal therapy are still unclear. According to Vankar et al.,7 the number of people who used herbal products in 2021 was 21%. It is unclear if these numbers have changed in the years since.
These studies highlight that many patients are using herbal products. However, it is unclear if patients are aware that herbal medications are not regulated, that they can have multiple potentially severe drug interactions,8 or that they should be reporting these medications to their prescriber and/or pharmacist. A 2007 study attempted to answer these questions, but it only focused on patients over the age of 60.9 For patients of today, the internet and social media are platforms that contribute to the spread of information about herbal products among a greater variety of age ranges. However, this information is not always correct and can be very misleading for patients. There can also be pressure from social media to use more natural medications over “unnatural” options. All of these changes mean it is also unclear which demographic of patients is more likely to use herbal products and for what reasons. This study was designed to address these knowledge gaps with the following objectives:
1. Characterize community pharmacy patients' baseline knowledge about, perspectives on, and use of herbal medications.
2. Examine to what degree patient demographics correlate with baseline responses.
3. Assess if pharmacist-led education about herbal medicines changed patient behaviors and perspectives.
Methods
Procedures
The study comprised a pre-education survey, an educational trivia game in the form of a popular gameshow (Jeopardy!. (1984). Syndicated Television. Sony Pictures Television), and a post-education survey. Surveys were completed on site and administered using Qualtrics software (Provo, UT), an online software platform used for data collection and analysis. This enabled the survey instrument to be distributed electronically to participants in the study. Copies of the surveys and educational game are available upon request. After completion of the study, participants received $5 added to their pharmacy rewards program account and cups/pens from the retail pharmacy and university. Responses from the two surveys were then compared to evaluate the impact of pharmacist-led education. Survey sessions were held in the lobby of five different retail pharmacies across the Oklahoma City metro area using a booth set up by the researcher. All materials and procedures used in this study were reviewed and approved by Southwestern Oklahoma State University’s (SWOSU) Institutional Review Board and by Walgreen Co. Participants were required to read, agree to, and sign an informed consent document stating the purpose, eligibility guidelines, procedures, risks and benefits, compensation, and voluntary nature of the study prior to completing the survey. Participants were also notified that completion of the surveys constituted consent to analyze their data as participants. All data were de-identified and reported in aggregate.
Pre-Education Survey
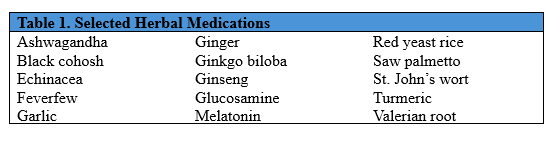
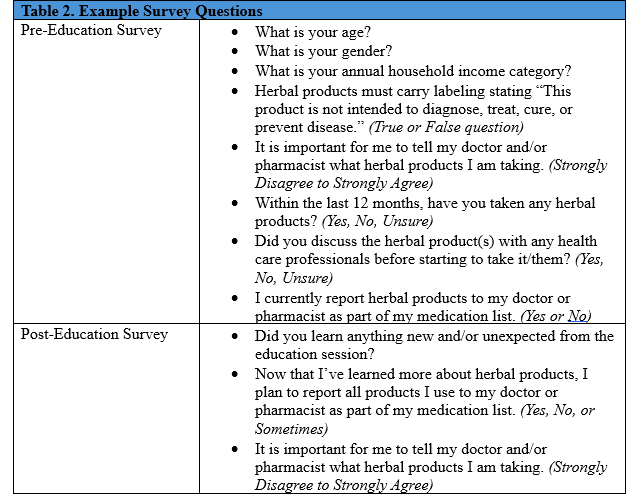
The initial survey for the study was developed to assess the participants’ perceptions, use, and knowledge of 15 commonly used herbal medications (Table 1). The survey used 28 questions including true/false, yes/no, Likert scale, and free response questions (Table 2). The surveys included the creation of a de-identified personal code that could be used to compare pre- and post-education survey answers. The survey also collected demographic information including age, gender, race/ethnicity, highest education level, annual income, and insurance status (Table 2). All questions on the survey were optional, and participants could withdraw from the study at any time.
Educational Session
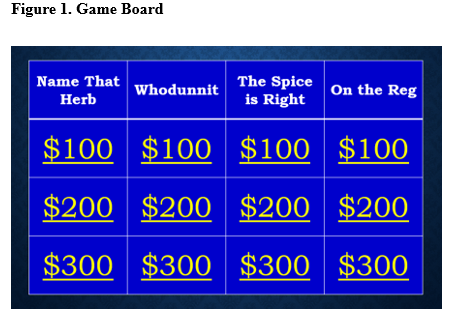
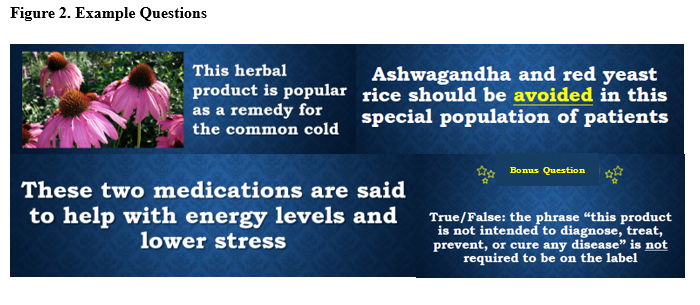
The educational session for the study was organized as a game of Jeopardy! (Jeopardy!. (1984). Syndicated Television. Sony Pictures Television) (Figure 1), which was completed live at the five participating pharmacies. This session lasted approximately 10-15 minutes depending on how engaged the participants were with the game, although engagement was not specifically measured. Topics included 15 commonly used herbal medications; health claims, side effects, and drug interactions associated with those medications; and regulation and labeling requirements for herbal supplements (Figure 2). The session included a question worth up to double the points to add excitement to the game, and a final question that assessed participant understanding of the importance of reporting herbal medications (Figure 3). After the session was completed, the primary researcher answered questions for participants and offered educational leaflets on each of the herbal products discussed; these were provided by UpToDate Natural Products database (Natural Products Database. UpToDate Inc.; 2024. Updated July 18, 2024. Accessed July 18, 2024. https://online.lexi.com.).
Post-Educational Survey
After completing the educational game, participants were asked to complete a second survey. This survey asked if they felt that the education session and content provided were beneficial, if they planned to report herbal product use to their prescribers in the future, and repeated the Likert scale perspective questions from the initial survey (Table 2).
Participation
Inclusion and Exclusion Criteria
Study participants were patients who were recruited in-store at five locations of a large-chain retail pharmacy across the Oklahoma City Metro area. Patients were eligible to participate if they were over 18 years of age and could speak and read English.
Recruitment
Data collection and recruitment took place from January 2025 to April 2025 on various days of the week and at various times. The original study design allotted for 10 study sessions, but an amendment was made to the design to allow 15 sessions. This change was deemed necessary after several sessions had been conducted with low participation. Flyer and prescription attachments were used to advertise the study, and patients who came to the pharmacy were verbally offered the opportunity to participate.
Measures
Survey validity was determined through piloting the surveys with several pharmacists, technicians, and laypeople. The survey was developed using common questions, as well as some that were adapted from Marinac et al.9 with permission. Surveys are available upon request.
Analysis
Descriptive and quantitative statistical analyses were performed on a per-protocol basis. All data were analyzed using JASP (Version 0.95.3) [JASP Team (2025), Amsterdam, the Netherlands] and were only included if participants completed the full study. It was calculated that 157 participants would be needed to reach a power of 80% to detect a difference in perspectives before and after education. As this study was completed within the scope of a pharmacy residency, time limitations necessitated adjustment of the sample size goal to 30 participants, enrolled over 15 study sessions. The results of the perspective, Likert-scale questions were analyzed using a Wilcoxon signed-rank test with a two-tailed alpha of 0.05. All other measures were analyzed using Chi-Squared tests with an alpha of 0.05.
Results
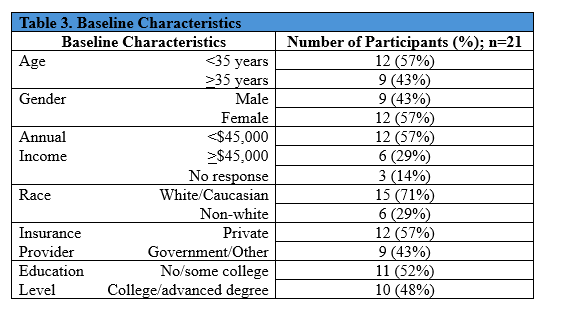
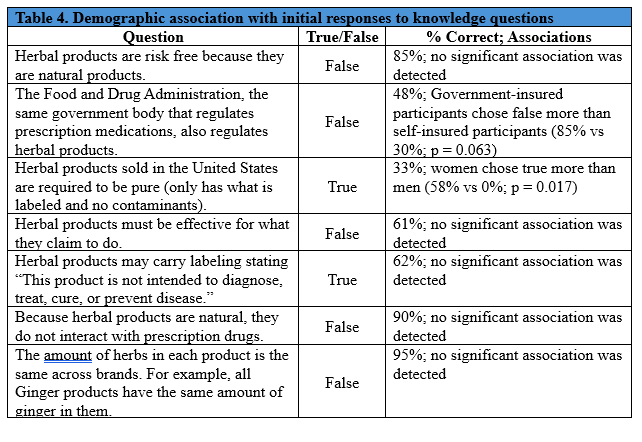
There were 21 patients who participated in this study. All patients who agreed to participate completed the full study and were included in the final data analysis. Baseline characteristics were uniformly represented, with race and annual income being the exceptions (Table 3). Patient race was primarily White/Caucasian, and the majority of patients had an annual income under $45,000. Twelve of the 21 participants (57%) had used herbal products in the past. Baseline responses to knowledge and herbal use questions were analyzed for any association with demographic information (Tables 4 and 5). Women were more likely to believe that herbal products are required to be “pure”, meaning low/no contaminants (58% of women vs 0% men believed this to be true; p = 0.017). It was found that patients over the age of 35 were more likely to use herbal products as compared to younger participants (77% vs 25%; p = 0.048), and those who had attained a college degree or higher were more likely to report herbal use to their provider (57% vs 0%; p = 0.038). There were no other significant correlations between patients’ demographics and knowledge/use of herbal products.
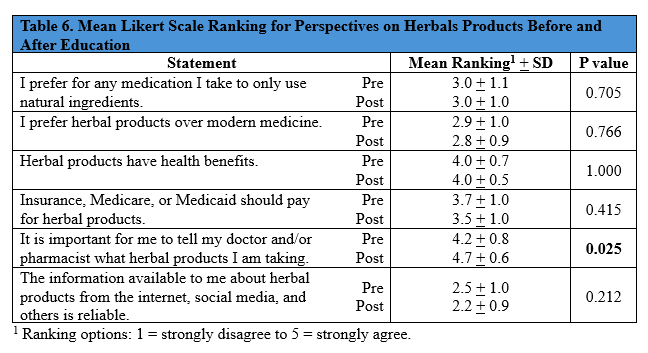
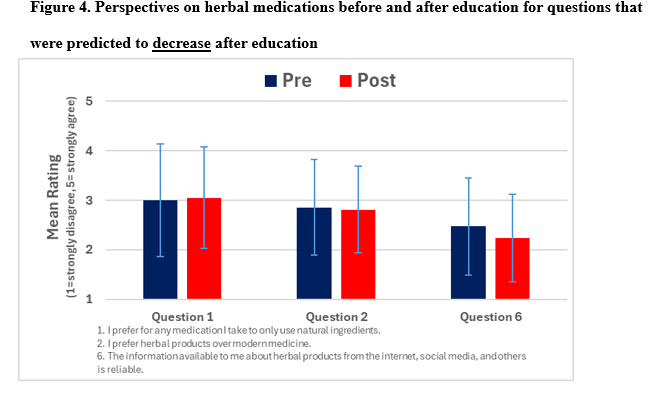
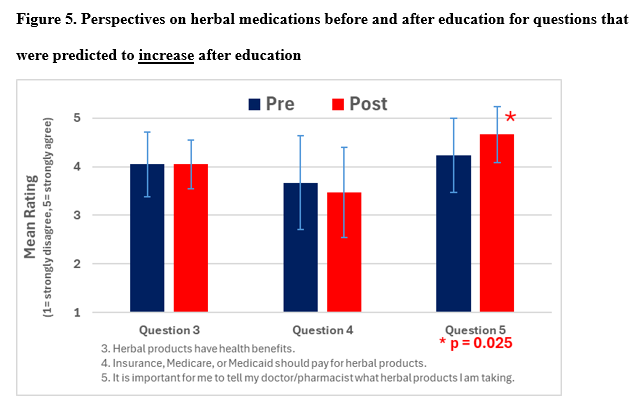
Prior to the educational game, only five of the 12 participants who used herbal products had reported them to their provider. After the educational game, 11 of those 12 said they would start reporting herbal use, and 19 of the total 21 participants said they would report any herbal use going forward. Additionally, patient rankings of the Likert scale perspective questions were compared to their responses prior to the educational game, and there was a statistically significant increase in the perceived importance of reporting herbal product use to a provider
(p = 0.025; Table 6, Figures 4 and 5).
Discussion
Herbal product use was stated by 57% of the study participants, supporting previous findings that there are many patients in the community pharmacy setting who are using herbal products. However, less than half of those participants were reporting herbal product use to their providers, highlighting the need for education in this area. Additionally, demographics including age, gender, annual income, insurance status, and education level have the potential to affect how patients perceive and use herbal products. Ensuring that patients are well educated on herbal therapies and that they are using them safely is not often at the forefront of a pharmacist’s duties. However, the results of this study indicate that pharmacist-led education can have an influence on how patients think about and use herbal products, thus reinforcing the need for pharmacists to include herbal therapies in their counseling and medication reconciliations. The study was able to detect a statistically significant change in opinions on reporting herbal medication use before and after education. Additionally, all of the participants were able to correctly identify the answer to the final question, indicating an understanding of the importance of reporting herbal product use. However, the study would need to be repeated over a longer time period and at multiple sites to provide a larger sample size to truly determine significance.
This study had several limitations. The sample size was not large enough to meet power, which may limit the ability to make associations with a larger population based on the findings. Additionally, the short study period limited recruitment of participants. An entire study session took approximately 20 minutes, which is a time commitment that could have limited patient willingness to participate. The study was also completed at only one chain community pharmacy, which could skew the sample as it is not representative of patients at different types of pharmacies. The study was designed to account for this limitation by hosting study sessions at several different pharmacy locations that were chosen to ensure that there was an adequate variety of races, ethnicities, education levels, and other demographics. There may have been unintentional self-selection bias, whereby patients who used herbal products were more likely to participate. Furthermore, the study design was based on self-reported behavior, which was not validated. Lastly, patient adherence to reporting future herbal use could not be assessed for this study.
The study also had several strengths. For example, the educational game was well organized, and the primary researcher received positive verbal feedback about the game from the majority of participants. Participants particularly liked the format of the education session and said that they felt they had learned while having fun. Additionally, the baseline characteristics were evenly represented among participants, with only a few exceptions. All participants who started the study went on to complete the study and were, therefore, included in the final evaluations. Finally, this study adds to the literature available on the topic of patient knowledge, perspectives, and use of herbal medications.
In older studies of herbal products,4,6 herbal product rate of use in the prior year ranged from 17-33% of patients. In contrast, this study identified that 57% of patients had used herbal products over the similar time period of a year. This supports the possibility that many more patients are using herbal products than previously reported. If the results of the knowledge questions (Table 4) are compared to the similar questions asked by Marinac et al.,9 patients today seem to be slightly more educated regarding herbal products. This is illustrated in that 66% of patients in 2007 believed that herbal products posed no risk;9 whereas, 85% of patients in our study correctly identified that herbal products are not safe just because they are natural. Another area of contrast with previous studies is the percentage of patients who reported herbal product use to their providers. This study found that 41% of patients who had used herbal products had also reported that use; whereas, Gardiner et al.6 found that only 18% had reported their use, although they only asked patients about reporting in a much shorter time frame (during a recent hospital stay). However, there are also areas where patient knowledge appears to have remained the same, with approximately 60% of patients from both studies falsely believing that the FDA regulated herbal products in the same way as prescription medications.9 When these comparisons are looked at as a whole, this study seems to have provided new perspectives on how patients use and report herbal medications and what they know about those medications. However, these results are ultimately difficult to directly compare due to differences in study design and the limited participation in this study.
Conclusions
This study attempts to address the knowledge gap in patients who may be using herbal products without reporting them to their healthcare provider or pharmacist. Findings demonstrated that there are demographic associations that may affect herbal product use and knowledge, as well as a statistically significant increase in recognizing the importance of reporting herbal medications to a provider after education was provided. Pharmacists can have a positive impact on comprehensive patient care, which includes the use of herbal therapies. While these results are limited due to a small sample size and should be interpreted and applied with caution, they indicate that pharmacist-led education has a key role to play in patient health with relation to herbal supplements.
References
1. Ashwagandha. In: Natural Products Database. UpToDate Inc; 2025. Updated August 23, 2024. Accessed July 29, 2025. http://online.lexi.com
2. St. John’s Wort. In: Natural Products Database. UpToDate Inc; 2025. Updated July 24, 2024. Accessed July 29, 2025. http://online.lexi.com
3. Food and Drug Administration. FDA 101: Dietary supplements. U.S. Food and Drug Administration. Published June 2, 2022. https://www.fda.gov/consumers/consumer-updates/fda-101-dietary-supplements
4. Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002-2012. Natl Health Stat Report. 2015;(79):1-16. Accessed July 16th, 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4573565/
5. Nahin RL, Stussman BJ. Expenditures on Complementary Health Approaches: United States, 2012. Natl Health Stat Report. 2016;(95):1-11. Accessed July 16th, 2025. https://www.cdc.gov/nchs/data/nhsr/nhsr095.pdf
6. Gardiner P, Sadikova E, Filippelli A, White L, Jack B. HHS Public Access Medical Reconciliation of Dietary Supplements; Don’t Ask, Don’t Tell. Patient Educ Couns. 2015;98(4):512-517. doi:https://doi.org/10.1016/j.pec.2014.12.010
7. Vankar P. Adults Who Used Alternative Medicine Treatments U.S. 2021. Statista. Published November 29, 2023. Accessed July 16th, 2025. https://www.statista.com/statistics/1341758/us-adults-who-used-select-alternative-medicine-treatments/
8. U.S. Food and Drug Administration. Mixing Medications and Dietary Supplements Can Endanger Your Health. U.S. Food and Drug Administration. Published 2019. https://www.fda.gov/consumers/consumer-updates/mixing-medications-and-dietary-supplements-can-endanger-your-health
9. Marinac JS, Buchinger CL, Godfrey LA, Wooten JM, Sun C, Willsie SK. Herbal products and dietary supplements: a survey of use, attitudes, and knowledge among older adults. PubMed. 2007;107(1):13-13. Accessed July 16th, 2025. https://digitalcommons.kansascity.edu/cgi/viewcontent.cgi?params=/context/facultypub/article/1340/&path_info=10.7556_jaoa.2007.107.1.13.pdf